This post presents water, sanitation and hygiene (WASH) interventions as a cause area.
WASH is a huge global problem, with 2.2 billion people lacking access to safe drinking water. About 1.5 million people die from diarrheal diseases and WASH is a very pronounced risk for death in children under 5. Yet, many of these deaths are largely preventable with basic treatment and sanitation measures.
Up until very recently, WASH interventions were not considered cost-effective but key new evidence has emerged and has made this stream of programs worth re-evaluating.
Chlorine treatments of water are impactful, cost-effective, rigorously evidence based, and deserving strong financial support.
There are other promising WASH interventions, such as hygiene promotion, that should be further explored and potentially supported.
WASH interventions may be particularly effective when their impact on varied health and economic outcomes is considered.
Although water and sanitation systems are forecasted to improve globally over time, when considering political and military conflict, as well as climate change, there are high risk areas where WASH interventions will be crucial and continue to be highly cost effective over extended periods of time.
WASH at a glance - UNICEF’S Key Facts
2.2 billion people around the world lack access to safe drinking water.
More than half of the global population lacks access to safe sanitation.
3 billion people do not have access to handwashing facilities with soap.
673 million people practice open defecation.
Children are at risk of deadly consequences of unsafe water, sanitation and hygiene (WASH). Each day, over 700 children under age 5 die of diarrhoeal diseases due to lack of appropriate WASH services.
Children in areas of conflict are nearly 20 times more likely to die from diarrhoeal disease than from the conflict itself. (Source)
What do we know about WASH?
WASH diseases & interventions
WASH interventions commonly include water and soap provision, water treatments (most commonly through chlorine), infrastructure and building improvements (e.g. plumbing, latrines), as well as knowledge, attitude, and behavior change programs.
In terms of diseases, WASH interventions can target diseases with cases in the billions per year. Summarizing from Montgomery & Elimelech, these include:
waterborne diseases (caused by contaminated water, e.g. cholera)
water-based diseases (caused by parasites in intermediate organisms living in water, e.g. schistosomiasis)
water-related diseases (diseases linked with the life cycles of insects that live or breed in water, e.g. dengue fever)
excreta-related diseases (those caused by contact with pathogens breeding in excreta, e.g. trachoma)
diseases relating to water collection and storage (such those caused by poor handling, container contamination)
toxin related diseases (caused by harmful bacteria like cyanobacteria, e.g. hepatic illnesses).
Fewtrell et al. (2005) carried out a systematic review and meta-analysis reporting a positive effect of WASH interventions on mortality. All interventions significantly reduced mortality with little variance in effect size (there was evidence for publication bias). Importantly, this review suggested that water quality interventions, in particular point-of-use water treatment interventions, were more effective than previously thought. Interestingly, some combined interventions (e.g. combining water and sanitation measures) were not more effective than single focus interventions
Clasen et al. (2015) report a systematic review based on 55 RCTSs, quasi-RCTs and controlled before-and-after studies. They report that interventions that distribute disinfection products at the household level (e.g. home chlorination products) can reduce diarrhea by 25%, although there was marked heterogeneity in individual intervention effect estimates. Point-of-use filtration systems have a larger impact, reducing diarrhea by 50%. Larger effects are noted in trials with higher adoption and adherence rate, as well as trials providing a safe storage container. There was insufficient evidence to conclude anything about the effects of source-based water quality improvements (e.g. protected wells, communal taps).
Kremer and colleagues’s recent (2022) meta-analysis identified 52 RCTs of WASH interventions and were able to meta-analyze 15 of those that reported child mortality as an outcome, indicating WASH interventions have a statistically significant impact in reducing mortality (roughly 25% reduction in all cause mortality). Further, this work provided key estimates of effectiveness, suggesting that the cost per 1 DALY averted thanks to water treatment is about 45 times lower than the WHO commonly used threshold of 1 x GDP per DALY. This research is a fundamental piece in considering WASH interventions as cost-effective.
Caveats and limitations
A key consideration in WASH interventions is the rate of adoption. Meta-analytic evidence from Classen et. al. (2015), Waddington et. al. (2009) & Arnold and Colford (2007) all suggest maintaining high adoption rates is essential to impact, and that higher adoption rates are linked to bigger impacts. It will be critical to assess interventions in terms of their capacity to achieve good user adoption. Some interventions seem highly cost effective while also maintaining room for further increases in adoption (this is further discussed below.)
An additional note is that, beyond measures of mortality, the majority of outcome measures in existing WASH interventions are self-report, typically self-reported diarrhea. Survey response biases are well discussed within the measurement literature and a commonly shared consideration is that objective estimates may differ from self-reported estimates. For instance, in the latest Cochrane review (that by Clasen and colleagues) self-reported diarrhea was the most commonly reported outcome, and it was considered at high risk of bias because of the lack of blinding in over 80% of the studies. Blinding is still uncommon in current WASH research and should be considered more widely, as well as other strategies to ascertain veracity of results. For instance, Ercumen and colleagues (2015) assess reporting bias by also collecting data on outcomes that are not expected to be impacted by their WASH intervention, such as skin conditions. These “control” outcomes differed slightly between control and intervention arm, indicating a low level of reporting bias. Relatedly, self-reported outcomes seem to correlate and track objective measures (e.g. objective measures of amount of chlorine in water) and so remain informative even if measurement improvements can still be made.
Cost effectiveness
Dispensers for Safe Water
Evidence Action’s Dispensers for Safe Water program provides chlorinated water dispensers in Africa and Asia – chlorine use for water purification is a WHO endorsed approach; chlorine can kill pathogens and help clean water and keep it safe for a few days of storage.
Evidence Action estimates they deliver a year’s worth of safe water access for less than $1.50 per person. Their coverage is over 28,000 dispensers providing chlorinated water to over 4 million people, including 570,000 children under 5 (for whom diarrhea is a significant risk for death).
An important finding of Kremer and colleagues’ work is their cost analysis specifically for Dispensers for Safe Water. They estimate a cost per expected DALY averted due to water treatment with this program can be as low as $39 or roughly $3000 to save a child’s life through water treatment. (NB under different models, 1 DALY can cost $52 or $59, so a plausible range to consider would be $40-60 per DALY)
Nevertheless, it’s important to recognize current limitations and potential for improvement. At present, Dispensers for Safe Water report a 60% average adoption rate. While this is a very good rate, this means there are still community members in the high need areas where Evidence Action works who have access to free chlorinated water but do not use the available dispensers or use it infrequently. Understanding barriers to access and adoption, and how to improve adoption rates can improve cost effectiveness. Investigation of this kind (e.g. promotion through WhatsApp of table top filters) is underway by other actors and varied work with similar aims should be encouraged.
Further, there is opportunity to scale up, and reason to think that scaling up can improve cost-effectiveness. Poverty Action’s write-up of this stream of work suggests that, if this intervention is scaled up, projections can be as low as a chlorine dispenser system costing $0.50 per person per year.
Coupons for Water Treatment
Another promising related stream of interventions provide free coupons or vouchers that can be exchanged for water treatment solutions (usually chlorine).
Kremer and colleagues review these types of interventions in their meta-analysis as well. In terms of cost-effectiveness, they estimate that 1 DALY averted due to water treatment via free coupons can be as low as $37, or again that it would cost roughly $3000 to save a life. (NB once more note different model specifications give two different point estimates for the cost of a DALY, at $50 and at $56).
One RCT in Kenya by Dupas and colleagues (in partnership with Kenya IPA) found that the free provision of water treatment solution through a voucher mechanism effectively screened 88% of people who would accept safe water under free provision but would not treat their water on their own (this was done through an objective measures test of households’ stored water for chlorine residual).
Dupas et al. compared three modes of water provision: cost sharing treatment (water provided at 50% discount price), vouchers treatment (12 vouchers for a 150ml water treatment solution each, one voucher redeemable each month), or free delivery treatment (2x500ml bottles of water treatment solution, one immediately given at sign-up and then the second at 3-5 months later). The voucher mechanisms achieved most of the benefits of free treatment, while eliminating the downside of potential wastage/ non-use that would be associated with including people who would not use the water treatment.
Nevertheless, it’s worth carefully looking at the rates of positive residual chlorine tests (used to assess whether people actually used the provided treatment). This 12.4% in the cost sharing group, 32.9% in the vouchers group, and 33.9% in the free delivery group (the latter two results did not differ significantly when comparing households at 3 or 4 months after enrollment). Importantly, these rates seem to fall below the adoption rate of 60% suggested by Dispensers for Safe Water, and highlight the need to better understand barriers and ways to improve adoption.
Caution should be applied as the % comparison may be unclear, the coupon program reports household-level percentages, but Dispensers may be reporting community-level adoption percentages. (The link Evidence Action refers to for the adoption reporting is currently broken and this is difficult to correctly ascertain).
Assuming the different % adoption rates are not precise but still somewhat informative, this may be an indication that the mode of provision of water treatment may be important. An advantage of Dispensers for Safe Water is that community members walk to their regular water source where dispenser buckets with chlorinated buckets are placed. Minimizing the disruption and behavioral change needed may be a way to promote higher adoption rates. At the same time, more explicit comparisons of different methods of administration, paired with participatory research, should be carried out in order to avoid paternalistic interventions and ensure recipient dignity and acceptability.
Carrying with the assumption that different % adoption rates may be informative, if indeed both vouchers and dispensers are comparably cost effective (vouchers slightly more so according to Kremer), it may be particularly important to examine level of consumption and waste regarding dispensers – what are the exact quantities of solution consumed and how much is not used; how often do containers have to be exchanged or repaired?
A more recent RCT by Dupas and colleagues (2020) in Malawi compares further modes of administration (coupon vs community health worker) and looks more carefully at non-adoption. In brief, the coupon program increased rates of chlorine-treated water consumption from 5% to 30% (constant over the follow-up period of 1.5 years). Further, the authors report that distribution of free chlorine through community health workers is less effective than a program providing monthly coupons for free water treatment.
Non-adoption of free diluted chlorine for water treatment was explained as driven by those households who already had a protected water source, as well those who reported disliking the taste of chlorinated water.
In this coupon intervention, it was estimated that $2.69 prevented one child illness.
Focusing more on cost effectiveness for this intervention, an average of 419 coupons/month were redeemed in a sample of 872 households, at a total cost of $258, i.e. $0.29 per household. Dupas et al. estimate that this was linked to 6,804 added households-days with treated water, thus yielding a cost effectiveness ratio of $1.13 per 30 household-days with treated water.
Cost estimates are based on the number of WaterGuard bottles distributed as well as their wholesale price (~$0.45 per bottle) as well as distribution costs (~$0.08 per bottle).
At present, most coupon programs providing water treatment seem to be delivered in a research context. The lack of clearly associated charities for direct donation is a challenge for donors. At the same time, this stream of research suggests a real opportunity to improve lives through cost-effective intervention. It may be possible to embed coupon programs within the work of already existing non-profits.
More broadly, both coupon programs and Dispensers for Safe Water share a core mechanism: the provision of chlorinated water. The distinct bodies of evidence for each should be seen as triangulation for the effectiveness and promise of this work. More direct comparisons of these two methods of delivery and understanding the characteristics driving different adoption of each can further enhance these interventions.
WaterAid
SoGive’s impact calculator suggests that donating £15 to the non-profit WaterAid can fund 1 sanitation intervention.
What do we know about WaterAid’s expenditure and interventions?
SoGive estimates that 42% of the direct expenditure at WaterAid goes directly to providing people with safe, clean water, sanitation, as well as hygiene education, and 37% of their expenditure further goes to “sector strengthening and capacity building” activities, such as advising local authorities on how to improve planning, coordination, performance monitoring, etc. 16% of WaterAid’s expenditure went to influencing water-related policies encouraging local authorities to prioritize WASH.
Recipients are most commonly in low and middle income countries, where the majority of interventions, at 46% are delivered to healthcare facilities, followed by people from local communities (43%), and children and teachers at schools (11% of all interventions).
SoGive estimates more concretely that it costs the non-profit WaterAid approximately £6 to provide one treatment of clean water or sanitation, though they caution this is likely an underestimate as WaterAid has local partners who are likely also involved financially supporting the interventions.
Knowledge gaps currently regarding WaterAid revolve around assessing impact from direct (rather e.g. policy) interventions on health outcomes, as well as impact from indirect (e.g. awareness campaigns) interventions. It is worth better elucidating the specific effectiveness of different intervention approaches.
Other promising & interesting work
(Note the Kremer review includes water interventions only, most of which are chlorination interventions. In this section I am trying to focus on other work that has not already been included in Kremer’s review or otherwise where I think still warrants highlighting. Further note that the majority of interventions or research listed below are somewhat outdated, coming from pre-2010s.)
Waddington and colleagues (2009) review some cost effectiveness estimates in the literature. They find that overall, hygiene promotion is most effective at $3 per 1 DALY averted, with sanitation interventions trailing at $11 per averted DALY, followed finally by sanitation construction programs reaching up to $270 per DALY. It’s likely that these estimates are outdated and perhaps imprecise, as logistics and distribution efficiency tend to improve over time.
In Kabul, the International Committee of the Red Cross helped deliver an intervention constructing new latrines or renovating existing ones. The range for cost effectiveness was from between $1800 to $4100 per averted death (based on 1 year of data, so the authors caution these may be conservative estimates).
In Ghana, the cost of delivery of the main hygiene promotion intervention (e.g. promoting hygiene behaviors like fecal containment and latrine use, hand washing with soap, drinking and storing water safely) is estimated at $90 per household, with cost effectiveness at $106.42 per capita of improved hygiene behavior.
In rural China (East Fujian), improvements in drinking water, health education and direction for villagers to improve health were associated with reductions in diarrhea incidence, with cost to benefit rations of 1:5 in 1991, 1:4.9 in 1992, and 1:6.5 in 1993. Earlier related work delivered in Henan, China, indicated that provision of central water supply and toilets showed reductions in morbidity rates by 54-79%. Both measures (water provision and toilets) cost ¥46 per capita. An annual benefit, from disease reduction and work force protection, was estimated at ¥23.5 per capita, estimating that the total costs would be paid in 2 years. A cost benefit ratio was estimated at 4.4 after 2 years.
Further considerations
Multi-outcome considerations
WASH interventions are typically evaluated in terms of direct health outcomes (e.g. prevention of diarrhea and associated deaths), but of course (as is true for many other health interventions), the outcome types may be varied - e.g. improvements in mental health, personal and regional safety, socioeconomic mobility.
Loevinsohn and colleagues’ review illustrates the importance of multi-outcome consideration specifically in the context of complex WASH interventions. The authors re-review an already existing Cochrane WASH review (27 papers) and suggest that when interventions are reviewed jointly from health and development perspectives, there is evidence for a wider range of impacts than initially considered from a health perspective alone. Further, the authors are able to suggest 6 new potential intervention mechanisms, as well as and considerations for how impact may be promoted or curtailed. It is important that such a comprehensive perspective is considered in future systematic reviews and intervention evaluations, both in terms of cost effectiveness calculations and in discussion about how to improve interventions.
Hutton & Haller’s 2004 WHO report on WASH interventions further provides valuable cost effectiveness information, particularly with a view of economic benefits (rather than just solely health benefits). At a broad level, they found that all surveyed WASH interventions were cost beneficial, and this was true for each region surveyed as well. In what the authors term ‘developing regions’, $1 investment in WASH projects was linked to a return in the range of $5-28. Economic benefits were produced largely due to the saving of time linked to better access to sanitation and water. Cost benefit ratios depended on region and intervention but ranged from 1.93 to 15.02. The paper provides further estimates for the value of time savings, annual time gain, productive days, healthy baby days, and school attendance gained thanks to WASH interventions.
Further, there’s evidence that WASH improvements are related to improvements in school performance, development and physical mobility milestones and mental health measures. These outcomes are generally rarely reported as primary outcomes and it is more difficult to ascertain causal relationships and robust effects due to lack of reporting and often imprecise measurement tools.
There’s some evidence to suggest that poor WASH conditions (including prolonged exposure to pathogens) can be a risk factor for child growth and development. Cumming & Cairncross (2016) argue WASH interventions have the potential to reduce stunting and should be deployed more widely. The body of related literature here is limited, in 2016 the authors were able to review two trials suggesting positive effects of WASH interventions for stunting prevention and three suggesting null effects, where low uptake and compliance were also reported. Further consideration of these outcomes is warranted.
Relatedly, Prüss-Üstün and colleagues examine disease burdens globally attributable to WASH. They consider “undernutrition and its consequences” as direct (attributable deaths resulting from protein energy malnutrition) and indirect (attributable deaths from increased susceptibility to diseases from undernutrition). They estimate that there is likely a huge number of child deaths, approximately 860,00 as of 2004, that are caused by malnutrition that could be prevented with improved WASH.
High risk considerations
While country-level water infrastructure and healthcare systems generally tend to improve (and we may think cost-effectiveness may decrease over time because of this), WASH interventions may become even more important and impactful for “high need” or “high risk” areas over time.
Specifically, high risk areas may be those that may be impacted negatively from climate change, in regards to the increase of warming, depletion of water sources, heat waves and need for improved cooling, as well those areas that may require additional water preparedness for disaster. Similarly, WASH interventions will likely continue to remain very effective and important in cases where scarcity of water may be a risk factor for political and military conflict.
It’s important to also know that individual characteristics, such as age and gender, may be important and may also intersect with context and water security.
Negative income shocks, environmental disruptions and instability can be a particular risk factor. It’s likely that the Covid-19 pandemic has already exacerbated WASH insecurity for women and girls in low income countries (Adams, Adams, & Koki).
It seems plausible that considerations of high risk/ high need, as well as sustainability and adaptability, can be important to ensure interventions are cost-effective and those most in need are reached.
Next steps
Funding chlorine water treatment charities such as Dispensers for Safe Water.
Supporting entrepreneurs or charities who want to provide water treatment in other high need areas and communities.
Support regardless of method of delivery, given that there is strong evidence the mechanism of chlorine treatment is effective and robust to different distribution strategies.
Consider giving special consideration to those who are willing to test innovation (e.g. improving taste of treated water), novel distributions or otherwise address gaps (e.g. deliver at community or health centers, schools).
Funding research that better understands optimal delivery of water chlorination (e.g. through direct multi-arm comparisons) as well as barriers to access and ways to improve adoption rates (e.g. through recipient interview and participatory research).
Funding research that carefully considers high risk and high need areas, as well as research that includes a variety of primary and secondary outcomes beyond diarrhea and mortality (e.g. stunting, mental health, socioeconomic mobility).
Further careful consideration, research, and potential funding to hygiene promoting interventions.
Further careful consideration, research, and potential funding to latrine construction and renovation interventions.
Further careful consideration and contact with other charities in this sector with the aim of evaluating their cost effectiveness.
This post is co-authored with Ben Garfinkel. It is cross-posted from the CEA blog. A PDF version can be found here.
Summary: Some strategic decisions available to the effective altruism m...
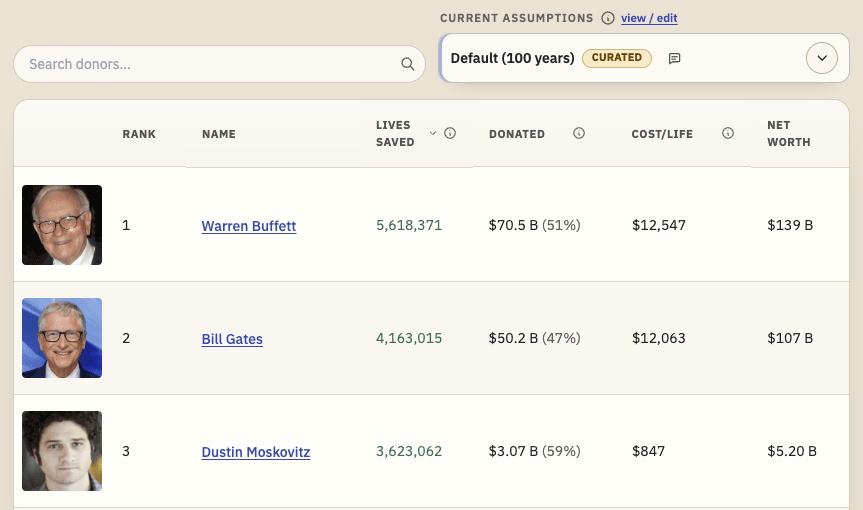
TL;DR: I'm releasing a website that ranks philanthropists according to EA principles and research, and allows users to re-rank the list using their own assumptions. I'd like feedback and help making it better. I'd especially like ideas for how to make the results more trustworthy. Funding may be available.
Crossposted to LessWrong.
...
Disclaimer: Although I work on the Groups Team at CEA, I’m writing this in a personal capacity, and this post does not constitute an endorsement by CEA.
Agency - the realisation that you really can just do things.
TL;DR
Biosecurity needs people (of any background) who are agentic and have a high execution velocity and track record....