You might want to reach out to Akhil Bansal, who was a Schmidt officer on AMR and now runs an AMR funding circle. He'll be very up to date on this issue.
Thanks for writing this up; more reasons to be optimistic!
I’m less clear on this, but it looks like the next step is that the trial data will be reviewed by the WHO; I’m not sure if there’s room to speed that up or encourage recommendation of the new regimens to the extent it should be encouraged
Looks like the next step is an already-funded Phase III trial due to finish in mid 2025. Don't think there's much scope to speed that up, but looking at the number of regimens tested, it looks hopeful that at least one of them will end up being a cost effective intervention.
Ah—where are you seeing that? The endTB page mentions under "What's next?" the phase III endTB-Q trial, but that's for pre-XDR TB, with "results [...] expected in late 2024".
You're right, I picked up the endTB-Q trial expected to announce findings in 2025, but missed that endTB-Q had a different target (fluoroquinolone-resistant MDR-TB) and wasn't just a continuation of the previous tests with a different drug cocktail.
Tuberculosis: Prepare to fund new MDR-TB regimens?
This post is co-authored with Ben Garfinkel. It is cross-posted from the CEA blog. A PDF version can be found here.
Summary: Some strategic decisions available to the effective altruism m...
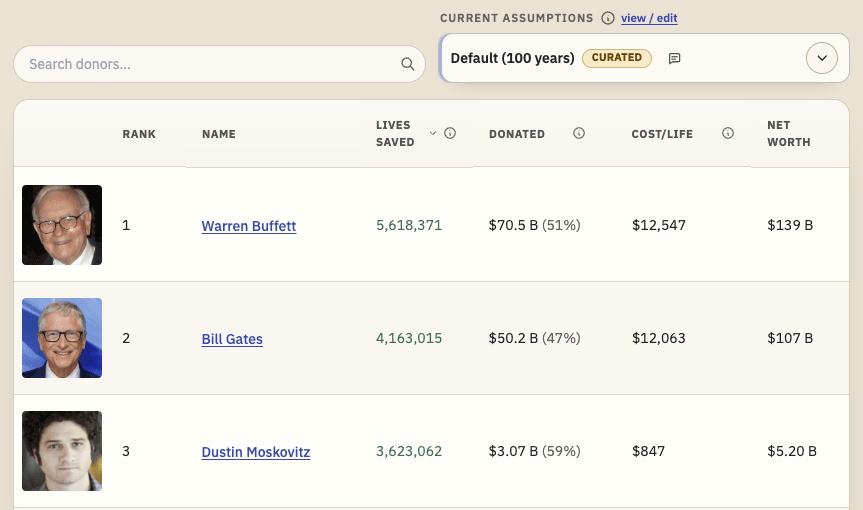
TL;DR: I'm releasing a website that ranks philanthropists according to EA principles and research, and allows users to re-rank the list using their own assumptions. I'd like feedback and help making it better. I'd especially like ideas for how to make the results more trustworthy. Funding may be available.
Crossposted to LessWrong.
...
Linkpost for my Substack piece, lightly adapted. Disagreement very welcome.
What happened
Coefficient Giving (cG) announced a $1 billion gift to GiveWell on 23rd July. This increases a previous commitment of $175m for 2026. cG say this could be a one-off surge, but it has implications for other donors either way. Both organisations...
Epistemic effort/status: 5–10 hours of research, mostly answering questions raised by my attempt to write up the argument. Questions raised by those questions were not all answered, and my lack of background knowledge in the area means I might have blind spots that minorly or substantially affect my thesis. Still, I’d rather post this sooner than later, so am posting a version that will, hopefully, be the start of discussion about this topic.
Summary
November 2023 results demonstrate non-inferior shorter, less painful, less risky, more convenient, cheaper treatments, suitable for more people, for multi-drug-resistant tuberculosis. I would like to know about prior work in this area, and suggest more investigation to determine if providing such treatments is cost-effective.
Background: The endTB results
MDR-TB refers to tuberculosis which is resistant to the two most powerful tuberculosis drugs, rifampicin and isoniazid, while RR-TB refers to tuberculosis which is resistant to rifampicin.[1] According to the CDC (2016), every year “nearly 500,000 people become sick with MDR TB, leading to approximately 200,000 deaths”. Active tuberculosis in general has a mortality rate around 70%, as noted by prior art on this forum.
Thanks to John Green’s YouTube video “MASSIVE Tuberculosis News”, I found out about the endTB trial results released in November 2023. The endTB trials tested new regimens of existing drugs and found that most of the new regimens—which are shorter (9 months compared to 18–24 months)—were at least as effective as the standard of care. Crucially, they’re also potentially much cheaper—two are less than $400 per course. A full summary in this table:
(There is also an all-oral 6-month regimen called BPaLM/BPaL introduced in 2022, but it’s not recommended for, among others, people who are under 14 or pregnant.)
The endTB documents also say the new regimens are appropriate for children, adolescents, adults, and pregnant people, as well as for those who have common comorbidities such as AIDS, diabetes, or hepatitis B/C.[2] Additionally, endTB regimen 5 (which is not clearly non-inferior, but whose use is ‘supported’ by the trials) doesn’t contain the medications bedaquiline or linezolid (“at least one of [which] is in every current World Health Organization-recommended regimen for MDR-TB”), which makes it a potential option for people who can’t take those medications.[1]
Cost-effectiveness
I think there are two main counterfactuals to consider here:
Someone who would otherwise not get treatment gets treatment (e.g., because the new regimens are cheaper and thus made available or because they’re easier to implement); this person has a high likelihood of dying without treatment, so the treatment likely saves eir life
Someone who would have gotten the current standard of care gets one of the new regimens instead → cheaper; the patient will have higher QoL and experience less injurious side effects; the regimen is easier to comply with and the patient is more likely to complete treatment (→ lower risk of increasing the prevalence of multi-drug-resistant TB)
Even though I expect the new regimens’ cure rates will probably be closer to those of the current standard of care, the substantial cost, quality of life, and duration improvements suggest to me that action and/or philanthropic expenditure in this area could be cost-effective. I suspect a decent number of people who wouldn’t start/complete the current treatments would complete the new treatment (because, e.g., the duration, pill burden, side effects, &c. are lower), meaning providing them with medication could save their lives compared to the counterfactual.
Thus, while I don’t have much expertise in GiveWell-style analysis, unless I’m missing something crucial, providing relatively effective <$400 treatments to people who are otherwise likely to die[4], even if we have to pay for several treatments to save one statistical person who would’ve died, seems to have the potential to be on par with estimates like the $3000–5000 to save a statistical life via insecticide-treated bed nets. (This estimate doesn’t take into account costs of distribution, potential expense increases to deal with greater numbers of people receiving treatment, or funding shifts.)
(While I haven’t done the whole calculation, we’d want to take into account the number of treatments distributed, the number of those that are actually completed, whether each person treated would’ve received a different treatment or no treatment at all, and mortality/QoL with different or no treatment.)
Finally, the QoL effects of the new regimens stand on their own (although I have less confidence in cost-effectiveness here): for instance, there’s an angle from which replacing current treatments with new ones prevents cases of deafness that would otherwise arise from the current treatments.
Caveats and thoughts
Much of MDR-TB doesn’t get diagnosed and treated at all (contributing to the mortality rate), so maybe there are even cheaper interventions at other bottlenecks, e.g., helping people to start/complete treatment. Another hat tip to tuberculosis prior art on this forum, which highlights mass case detection with an effectiveness of one death averted per US$877 spent (with the cost being money being spent on hiring health workers).
All of the non-inferior regimens were around 85–91% effective, but the control looks to have been around 80% effective,[1] whereas according to Wikipedia (which cites a 2014 source), the standard of care “can approach [a] 70%” cure rate. This suggests to me that 80–91% efficacy will probably not be seen in the wild; still, the regimens are non-inferior and the other advantages stand on their own.
This is pretty speculative, but more courses probably means more unfinished courses, which could increase the risks of more drug-resistant TB in the future, although on the other hand cured MDR-TB cases which then don’t develop/fuel further resistance push against that.
Conclusion
I’m less clear on this, but it looks like the next step is that the trial data will be reviewed by the WHO; I’m not sure if there’s room to speed that up or encourage recommendation of the new regimens to the extent it should be encouraged. If/once the regimens are approved, it seems to me there will be opportunities to fund the new courses and possibly to increase awareness of them as options among doctors (though maybe they’re already keeping up?) and among potential patients. In the meantime, I would like to see any existing research on this; from my POV, it looks like there’s more investigation to be done regarding the potential cost-effectiveness of funding the new regimens, as well as of other interventions for tuberculosis.

You might want to reach out to Akhil Bansal, who was a Schmidt officer on AMR and now runs an AMR funding circle. He'll be very up to date on this issue.
Thanks! I don't use LinkedIn—is it within the bounds of propriety to tag his EA Forum account here?
You can always reach out via the forum!
https://forum.effectivealtruism.org/posts/W93Pt7xch7eyrkZ7f/cause-area-report-antimicrobial-resistance