Comments
Lafiya distributes self-injectable contraceptives across rural northern Nigeria. This post is meant to give a review of our work in the last year, present Rethink Priorities’ updated cost-effectiveness model on our work, and highlight our plans for the upcoming 18 months.
GiveWell's recent report highlights that they consider family planning interventions highly promising, with a cost-effectiveness bar of $20 per counterfactual year of protection for a couple (CYP); that is, a year of contraception that would not have happened otherwise. According to our most recent external cost-effectiveness analysis, conducted by Rethink Priorities, Lafiya can deliver a counterfactual CYP for $8, making us more than twice as cost-effective as GiveWell’s bar. Their CEA estimates our direct delivery work to be between 35-42x as cost-effective as cash transfers. We aim to reach 500k women with family planning by 2026. Alongside our direct work, we are currently focused on strengthening the contraceptive supply chain in Nigeria, integrating more deeply with government systems, and expanding into new areas. We’re looking to close our 2026 funding gap and would love to hear from you if you want to contribute to closing it.
We previously introduced Lafiya on the EA Forum here and were incubated by Charity Entrepreneurship in 2023.

In Nigeria, women have a 1 in 22 lifetime chance of dying from childbirth-related complications. Roughly 75,000 women in Nigeria die every year while giving birth or shortly after. The majority of these deaths are preventable with accessible family planning and maternal health care. But in rural Nigeria, only 30% of women give birth with a skilled provider present, and only 10% of women use modern contraceptives. In many places in the rural North, even fewer women use modern contraceptives (e.g. 3% in Kebbi, 3.5% in Jigawa). This means women give birth frequently (with total fertility rates in our operating states between 5.2 and 7.6 children per woman), and they are left without appropriate healthcare to plan their families or take care of their children. Despite high demand (>20% of women in the north want to use family planning) and the well-established impact of family planning, millions of women remain without access to the information and services they need to make informed choices about their health and futures. Donor exits (e.g. USAID and various other national governments) have exacerbated funding gaps. Systemic obstacles bar women from accessing services. Family planning products are frequently out of stock, and there are few trained providers who can give accurate information with due consideration of women’s concerns. This gap persists not due to low demand, but because existing supply systems face significant inefficiencies that limit consistent availability of family planning commodities at the last mile, particularly in hard-to-reach or underserved areas. Strengthening community-based distribution complements government efforts by extending reach and improving continuity of access. In Northern Nigeria, where coverage is low and demand is substantial, the opportunity to deliver cost-effective services is particularly strong.
Our users who want to learn how to self-inject and can demonstrate the correct technique receive three more doses to take home for a year of contraceptive protection
To address these access barriers in a scalable and cost-effective way, we designed an approach centred on community-based last-mile delivery. At Lafiya, we're on a mission to make contraception accessible to anyone who needs it and wants it - no matter where they live. Our approach is simple yet innovative: we train a network of dedicated female health professionals (we call them Lafiya Sisters) who are living in rural communities. Our training provides them with information to counsel women on family planning methods, and we provide them with an innovative injectable contraceptive: DMPA-SC. DMPA-SC is a locally highly sought-after contraceptive that is easy to distribute. It lasts three months, costs just $0.85 per dose, does not require a cold chain, is highly effective and has few side effects. Crucially, women can self-inject it: a health provider teaches women how to self-inject during a first visit, and subsequently gives women three doses to take home, so they can self-manage their contraception for the rest of the year. This commodity was specifically designed for remote, low-resource settings, exactly like rural Nigeria.
So why did we design our model in the way we did? To answer that question, we need to take a deeper look at the main barriers to family planning:
Lafiya’s model addresses all three barriers. We bring commodities directly to the point of distribution, strengthening the supply chain and ensuring stock is available continuously with our Lafiya Sisters. Training increases the number of health workers available to conduct counselling about various contraceptive methods. During their counselling, they are specifically prompted to address myths and misconceptions. We developed a digital counselling tool that provides Lafiya Sisters with personalised prompts, helping them respond to client questions and concerns in real-time with supportive, accurate information.
The Lafiya Sisters work for the government in primary health clinics, and they also go out into the field on outreach visits, reaching communities that are cut off from the current healthcare system. This works: almost half of the people we reach (46%) have never used contraception before. We now serve approximately 30,000 women per month and keep on growing our scale.
A Lafiya Sister discusses different family planning options and dispels myths about contraception with a local community of rural women
Hafsai (27) from Jigawa state wanted to space her pregnancies, but had no access to family planning because she lives far from the nearest clinics and cannot afford to get there. Her frequent and unplanned pregnancies made it difficult to work and care for her children. During Lafiya’s community outreach in her village, Hafsai learned about the opportunity to take DMPA-SC from the Lafiya Sister, and since she self-injected, she now has contraceptive cover for a year. Zainab says, “I used to cry when I missed my period because I knew I couldn’t handle another child. Now, I can sleep with peace of mind.” She can take care of her six children and provide for them without worrying about the future.
Hafsai and her husband in Jigawa state during one of Lafiya's outreaches
While our early focus was solely on reaching users directly, it became clear that sustainable impact required addressing broader structural bottlenecks in procurement, financing, and data visibility. In addition to our last-mile delivery work, we engage in strengthening the Nigerian health system and the contraceptive supply chain. Specifically, we have observed the following bottlenecks in the supply chain, impeding last-mile distribution:
Right now is a pivotal time for implementing a sustainable approach to family planning. The recent exit of USAID has highlighted the sector’s over-reliance on donors, triggering a major reset.
As a result, our work focuses on strengthening the landscape in several crucial ways:
Klau presenting about Lafiya’s work and digital strategy at the Technical Working Group, a major coordination platform with national policymakers
Our approach is highly cost-effective: based on current assumptions and modelling inputs, Rethink Priorities’ CEA estimates that with our direct delivery model, we are able to cover one counterfactual year of contraception for $8 this quarter (Q3 2025). For reference, GiveWell’s recent report states that programmes providing a counterfactual year of contraception for under ~$20 could be competitive with their top charities.
Our programmatic cost for one year of contraceptive access (CYP) is $4.85. This includes contraceptive and pregnancy test procurement, Lafiya Sister stipends, field staff cost, and set-up cost & training. The majority of this cost (74%) is DMPA-SC procurement. In our current model, we directly procure the contraceptives to ensure consistent supply and expand access where it is otherwise limited. Over time, our aim is for the government to take on procurement and running costs, a shift that supports long-term sustainability. We are primarily focused on driving down programmatic costs, since these will be the primary cost at scale. In this stage of growth, we consider it justifiable to invest more into our operations and M&E to iterate our model towards the best possible version before deploying at scale. Philanthropy can fund the set-up; government can take on running costs to ensure long-term sustainability.

The benefits of family planning go beyond direct health outcomes for women - the flow-through effects on their families and communities make this intervention particularly cost-effective
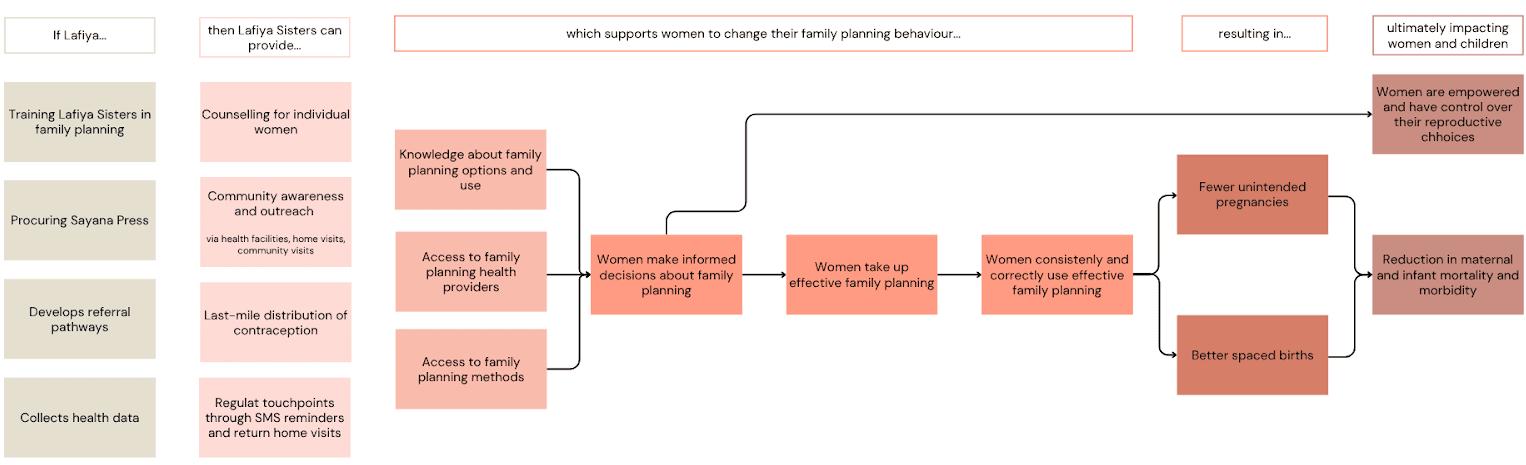
Our theory of change (below) is based on robust research conducted in the area of family planning. From literature, we see that consistent use of family planning is a highly effective method to reduce maternal deaths: an analysis of 172 countries shows that contraceptive use prevented 44% of maternal deaths, meaning the global maternal death rate would have been 1.8x as high without family planning. Women with an unmet need for contraception account for 84% of unintended pregnancies. Satisfying unmet need for family planning could lead to an additional reduction of 29% of maternal deaths.
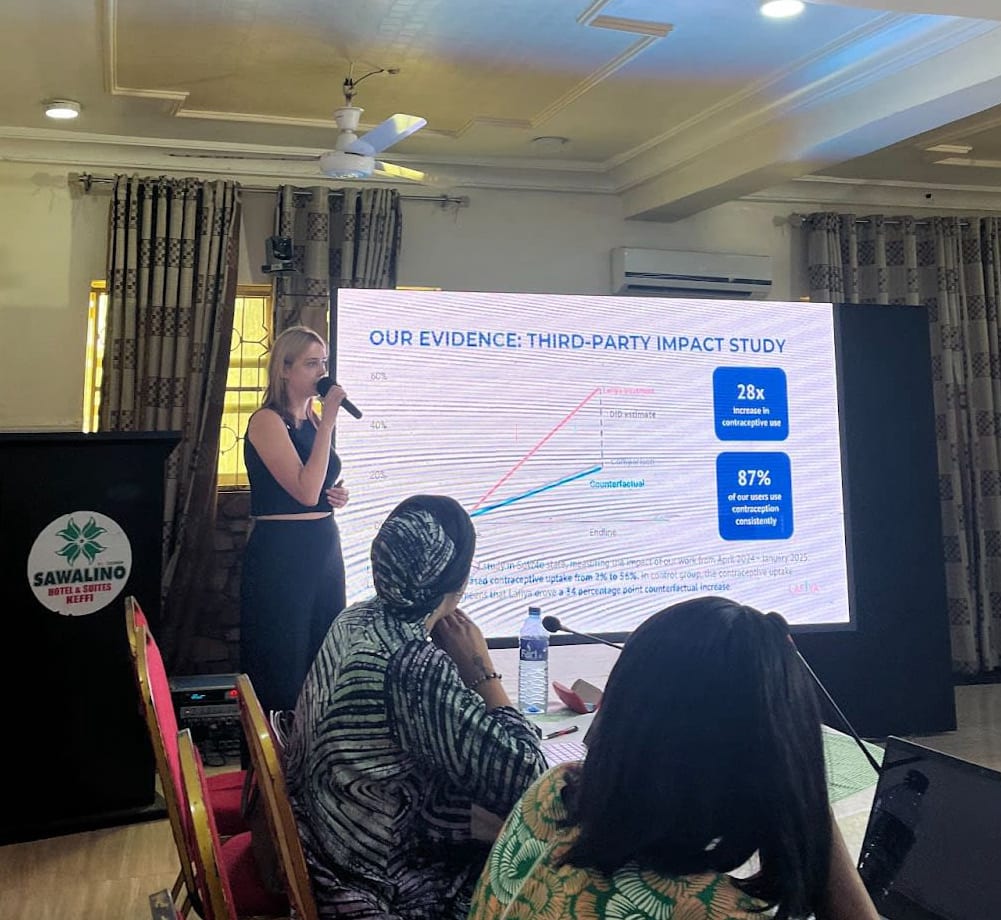
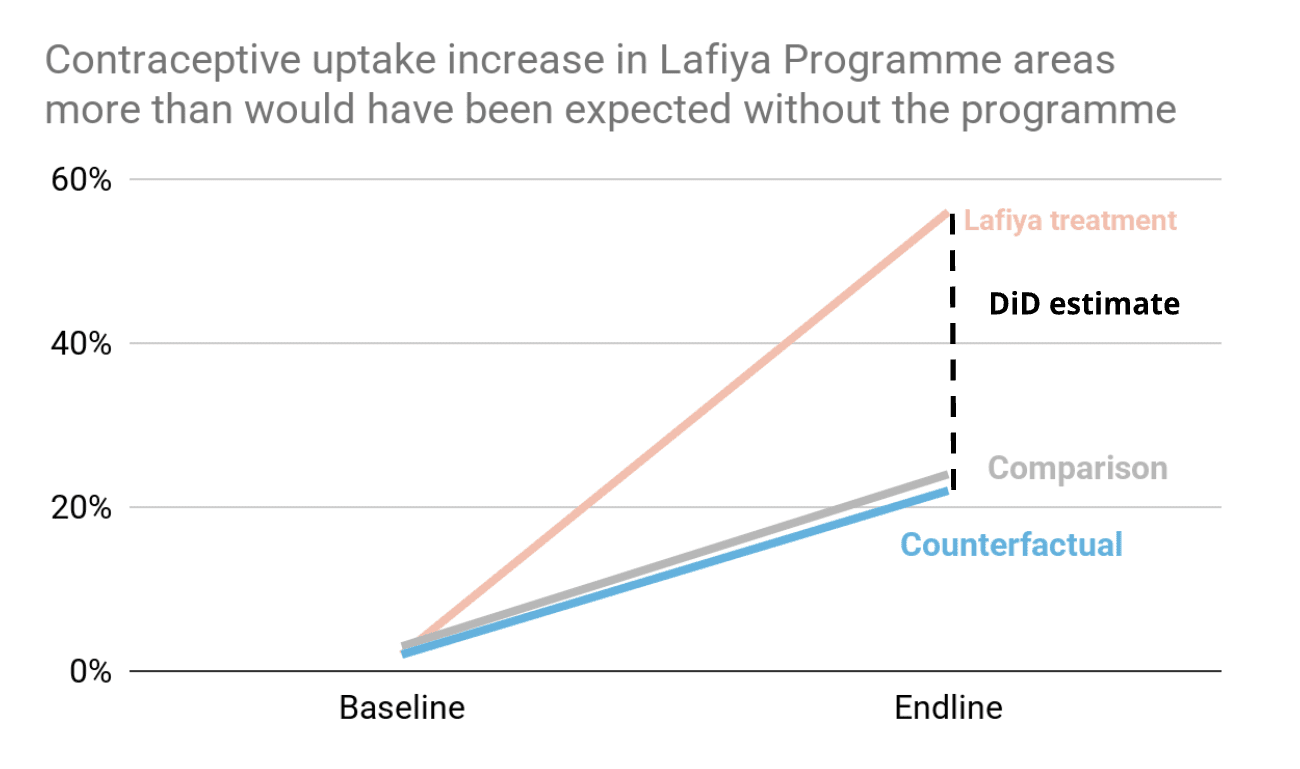
The link we were most uncertain about in our Theory of Change is whether our specific intervention effectively removes the access gaps to trained providers and contraceptives, and translates into increased contraceptive uptake. This is why earlier this year, we conducted a field study in Sokoto state. Our field study compared areas with and without Lafiya’s programme over an eight-month period (April 2024-January 2025). The main outcome: in the Lafiya programme areas, contraceptive use increased from just 2% to 56%, which is a 28x (2800%) increase from baseline. In the control areas, family planning use increased from 3% to 24%. Our model estimates that without Lafiya's intervention, contraceptive uptake in our catchment areas would have increased from 2% to 22%. This means that our programme led to a counterfactual 34 percentage points increase in contraceptive use among women, within an eight-month time frame. Given the extremely low starting rates, we consider these results very promising.
Now that we have this result, an open question remains whether women actually continue using family planning consistently (the next link in the ToC). In the initial study, we see that 87% of women in Lafiya areas reported using their contraceptive method consistently. We see this as a sign that the characteristics of DMPA-SC align well with the needs of the target population. To follow up, we now plan to test these results further through longer-term evaluation and have planned a follow-up study for Q4 2025.
Although it was not a central outcome metric of the study, we also found that in our intervention area, the pregnancy rate at the endline was 6%, while in control areas it was 30%. We see this as a plausible indication that our model is effective at reducing the number of unintended pregnancies.
Our future monitoring and evaluation plans are dedicated to systematically moving toward longer-term health and autonomy results, with the next stage of evaluation examining the impact of our intervention on short-term births and averted unintended pregnancies.
We’re proud of Lafiya’s progress, but we also recognise the limits of what we know. Below are some of the key uncertainties and areas we’re actively investigating. We share these in the spirit of transparency and as an invitation for collaboration and learning.

The launch of our program in Kano and the training of new Lafiya Sisters, November 2024
We are now focused on:
We work closely with partners within the family planning and primary care ecosystem to coordinate our work and leverage respective expertise to advance those objectives.
We are seeking to close a $1.62 million funding gap on our $2.6M 2026 budget [note that we will edit this section regularly as new commitments come in, to give you an up-to-date figure]. We are very intentional about building sufficient runway: continuity of services is essential for our programme. Any interruption of family planning services can lead to immediate risk of unintended pregnancy, reversing months or even years of progress. We’ve also worked hard to build trust with users who rely on consistent access: service gaps would jeopardise this trust and undermine future uptake of services.
Funding would support:
We believe Lafiya represents a credible, evidence-backed bet for funders interested in high-upside opportunities within global health, aligned with the evolving thinking of organisations like GiveWell.
We welcome you to reach out if you are interested in speaking with us about helping us close our funding gap, partnering to increase our impact, or conducting research on our work.
Please email us at [email protected] and [email protected] to continue the conversation.
Our leadership team at EAG London in June 2025 - missing Miranda, our new Director of Advocacy