I work at Open Philanthropy on cause prioritisation and on our science giving, and I agree with the direction of your conclusion here from a “Global Health and Wellbeing” point of view (i.e. rather than a longtermist POV), that funding particular infectious disease R&D could be as or more cost-effective at averting DALYs as GiveWell top charities. Indeed I’d expand what you’re saying from vaccines to other global health R&D - new therapeutics, new low cost diagnostics, new mosquito control tools, etc.
I’m not sure what level of investment that might remain true at, and we’re always interested to explore which diseases and health technologies might be most worth investing in. If you (Josh) or anyone else reading this has more ideas on what directions to head, or are interested in global health R&D and just want to say hi, feel free to comment here or email me at jacob [at] openphilanthropy [dot] org.
(For other readers, I know Josh via his work at 1Day Sooner, and we fund 1DS, but I didn’t know he was going to write this post, and stumbled on it organically. I liked it, thanks for writing it Josh!)
Thanks for posting! I think sharing ideas like this is very valuable, and you give what looks to me like a good overview.
I think the "Gates and Wellcome already fund this" point is worth expanding on significantly before going any further.
How much do they fund it? What haven't they tried? These seem like important questions for gauging whether we'd expect an extra $X billion to be very useful here.
The Gates Foundation has donated a total of $4.1 billion to Gavi to-date, including $1.6 billion in 2020 for Gavi’s latest 2021-2025 strategic period. Through Gavi, the Gates Foundation has also funded AMCs, for example to expedite the development and availability of pneumococcal vaccines. In addition, the Foundation also funds vaccine development directly through its Global Health division, at an increasing rate. According to the latest published figures, the Gates Foundation donated $220 million to vaccine development in 2020, up from roughly $133 million in 2019 and roughly $94 million in 2018, which indicates that they also see vaccine R&D as an effective way to save lives. The focus is particularly on diseases in low-resource settings such as HIV or Malaria, which recently saw a big breakthrough, and on technical innovation and novel platforms.
The Wellcome Fund's initiatives include funding CEPI to help fill critical gaps within vaccine funding and R&D, working towards the acceleration of a universal flu vaccine, and supporting WHO to create R&D blueprints for tackling Lassa fever, Nipah and Ebola, among others. It is also active in supporting Human Challenge Trials by funding clinical sites and helping to build local research capacity. All in all, Wellcome’s charitable expenditure is much lower than the Gates Foundation’s. Without specifying how much money goes into which projects, the annual reports states that in 2020 GBP 15 million (~$20 million) were allocated to vaccines, down from GBP 17 million (~$23 million) in 2019 (see Full Report 2020, p. 37).
While Gates and Wellcome seem to have a comprehensive range of activities, they are only able to fund a small part of vaccine R&D. It can be assumed there’s quite a bit of way to go until we reach the point of diminishing DALY returns. Here’s a simple calculation: In the case of tuberculosis, where there is a 100-year-old vaccine that is quite ineffective, only $117 million went into TB vaccine research in 2019, against a target of at least $550 million (see p.8) per year to come up with a new, effective vaccine by 2025. So even if all of Gates’ and Wellcome’s vaccine funding in 2020 combined, around $240 million, went into TB vaccine research (which it doesn’t), there would still be a funding gap of about $200 million per year, or $2 billion per decade, and that’s just TB.
Thanks for sharing this Josh. Always pleased to see arguments for boosting investment in global health R&D. Our nonprofit pharma team is working to address some of the diseases highlighted above, from tuberculosis drugs to rotavirus vaccines to preventive drugs against worms (see our website medicinesdevelopment.com for a description on these areas or reach out to us via philanthropy at medicinesdevelopment dot com).
I liked this post overall, but I think it may be optimistic about the effect of challenge trials on speeding up vaccine development in a couple of the mentioned cases. I was in a malaria vaccine challenge trial 11 years ago, and if I remember correctly the same lab was also testing tb vaccines with challenge trials. I think challenge trials are a really good idea, but if they're already being used for some of the diseases mentioned then we don't have an opportunity to improve things much by funding more of them.
There are certainly places where HCTs aren't the right tool - and Josh suggested that several approaches are worth pursuing - but they do seem underused compared to their value, and they are almost unique in their ability to allow testing of certain vaccines. For instance, a universal influenza vaccine is difficult to trial naturally, because you can't see what it does or does not protect against, and you only get data about the variants circulating the current year.
And the existence of some HCT work doesn't imply that we're anywhere near to optimal level - yes, there have been a few hundred HCTs in the past 40 years, but they haven't been used much or at all for many diseases, sometimes for relatively justifiable reasons that I would disagree with, and other times for no reason other than no-one has done it. (There are also cases where HCTs are, in fact, actually unethical or impossible - for example, there are some bird flus that are 100% fatal when humans catch them, but which aren't human to human transmissible. But I'm leaving those aside for now.)
In any case, yes, this isn't a brand new idea, but neither were mosquito nets, direct cash payments, or treating schistosomiasis - but they are effective causes nonetheless.
I'm definitely in favour of further consideration of this. However, I'd like to see the case for curing infectious diseases considered alongside the case for researching anti-ageing interventions.
It seems plausible that developing a successful anti-ageing intervention (a) would have an impact larger in scale than one for infectious disease (because it would be cross-cutting against the risk of cancer, heart disease, stroke, dementia, worsening mobility etc) (b) is more neglected (unlike research into treatments for specific diseases of ageing) (c) would also reduce deaths from some infectious diseases (e.g. influenza, Covid) (d) is much more risky/uncertain in terms of tractability
Not opposed to EA anti-aging research, but my intuition would be targeting infectious disease allows for more rapid iteration and proof of concept because the solutions are easier to publicly demonstrate in the short term. So I think it provides better training for EA methods (which could in turn enhance aging research).
Also, infectious disease affects poor people disproportionately and as such there's more likely to be a market failure and undersupply of resources rather than aging, which is a proportional problem between the rich and poor.
Most likely infectious diseases also play a significant role in aging- have seen some research suggesting that major health inflection points are often associated with an infection.
I like your post and strongly agree with the gist.
DM me if you’re interested in brainstorming alternatives to the vaccine paradigm (which seems to work much better for certain diseases than others).
I don’t think it is actually a pessimistic paper for the pro-AMC case. The top-line result of “only 6 cents of additional R&D spending per dollar” is just part of the story. My summary of that paper:
Finkelstein finds large benefits (billions of dollars worth) from the increases in coverage paid for at only moderate (in the tens of millions $ range) cost. This is the “static benefit” of increasing vaccine coverage given the generally large benefits of higher vaccination rates.
Finkelstein looks at Hepatitis B and the flu vaccine more closely and basically concludes (A) that the induced increase in R&D for Hep-B was useless because the existing vaccine was already excellent (90% efficacy, few side effects), so it couldn’t be much improved upon, but (B) that the flu vaccine R&D was very useful, somewhere in the billions range, because it likely caused the development of the newer flu vaccine, which is apparently quite a bit more effective. This is the “dynamic benefit” of increased R&D causing an improvement in vaccine efficacy.
I think the take-away is that if AMC’s act like the instrument Finkelstein uses here, we shouldn’t expect an AMC to stimulate a lot more private pharma investment, but they could still be very cost-effective if they resulted in an efficacious vaccine or if they sped up rollout. Notably, speeding up rollout is basically what Finkelstein found happened with the Hepatitis B vaccine.
So AMC’s could still be very cost-effective if the vaccine developed is effective and/or roll-out is sped up, as in the GAVI Pneumococcus AMC case.
Another factor is that Finkelstein examined the effects of increased revenue on already existing vaccines, while the proposed AMC's would mostly be focused on new vaccines.
My guess is that if Finkelstein found a big dynamic benefit from more R&D in the flu vaccine case just by a moderate increase in vaccine efficacy, then going from 0 efficacy (no vaccine) to moderate/substantial efficacy (new vaccine with vaccine efficacy of 75%) would yield large dynamic benefits. But I might be misunderstanding this part- not super confident in this.
EA Should Spend Its “Funding Overhang” on Curing Infectious Diseases
This post is co-authored with Ben Garfinkel. It is cross-posted from the CEA blog. A PDF version can be found here.
Summary: Some strategic decisions available to the effective altruism m...
Disclaimer: Although I work on the Groups Team at CEA, I’m writing this in a personal capacity, and this post does not constitute an endorsement by CEA.
Agency - the realisation that you really can just do things.
TL;DR
Biosecurity needs people (of any background) who are agentic and have a high execution velocity and track record....
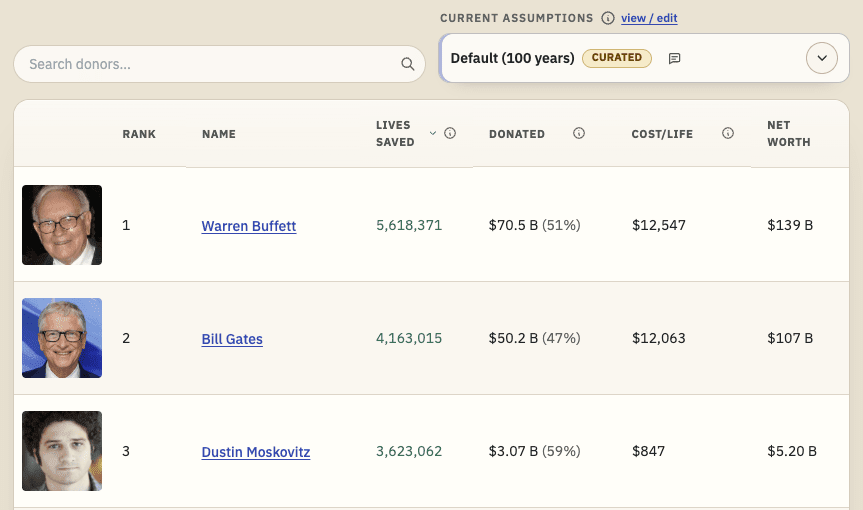
TL;DR: I'm releasing a website that ranks philanthropists according to EA principles and research, and allows users to re-rank the list using their own assumptions. I'd like feedback and help making it better. I'd especially like ideas for how to make the results more trustworthy. Funding may be available.
I recently built Impact List (impactlist.xyz), a site which ranks people by their positive impact via donations.
The goal is t...
1Day Sooner May Have been Wrong About COVID Challenge
Vaccines May Be Very Difficult to Develop
Vaccines Aren’t a Silver Bullet
Gates and Wellcome Already Fund This
Next Steps
Intro
There has been much discussion in the EA community lately of a “funding overhang” where there is more effective altruist money to spend than EA uses to spend it on.
As a nonprofit employee of 1Day Sooner whose salary is largely paid by various members of the EA community, the prospect of a funding overhang sounds too good to be true, but insofar as it does exist, I’d like to argue that a fair amount of this decade’s portion should be spent developing and deploying vaccines against infectious diseases.
Millions of deaths each year are caused by tuberculosis (1.4M), Group A Strep (500K), malaria (400K), influenza (300K), hepatitis C (300K), shigella (200K), and respiratory syncytial virus (160K). On certain reasonable assumptions, I’d argue they can absorb billions of dollars in GiveWell-charity equivalent funding over the next ten years. Beyond the object-level of saving millions of lives, developing effective vaccines to major diseases would benefit pandemic preparedness and EA’s political reputation in a way that could reduce existential risks long-term.
My expertise on vaccine development is at best incomplete, and I am biased because 1Day Sooner is raising money to work in this area. But the scale of the problem is large, multiple reasonable strategies exist to help address it, the timing is opportune, and the approach usefully diversifies EA funding strategies while complementing other long-term EA goals.
Tl;dr: If EA’s investing $10 billion in vaccination over the next ten years could save the equivalent of 3-5 years of disease burden of a disease like tuberculosis, it would represent a cost per disability-adjusted-life-year (DALY) saved of roughly $50-$85 (on par with GiveWell top charities). There are plausible mechanisms available to accomplish this, such as advanced market commitments, challenge studies, systems immunology research, and subsidizing mRNA vaccine manufacturing capacity. The effective altruism movement should quickly begin investigating this area more thoroughly and consider developing funding mechanisms commensurate with the scale of the opportunity.
Epistemic Status:I feel this makes a decent but simplistic default case that merits mild confidence in the absence of refutation (which I encourage people to do so as to sharpen the analysis).
Big Problem: Infectious disease is a big enough problem that a number of GiveWell’s top charities (e.g. Against Malaria Foundation and the END Fund) focus on mitigating its impact. Developing and deploying vaccines can dramatically reduce disease incidence in the long-run.
To give a sense of scale, here are the DALY’s lost annually to some vaccine-preventable diseases.
Annual DALYs Lost to Certain Infectious Diseases and Disease Categories (in millions)
HIV/AIDS
66.7
Malaria
55.8
Tuberculosis
40.3
Hepatitis C
12.6
Typhoid
10.6
Group A Strep
10.5
Schistosomiasis
3.4
Dengue
1.1
Diarrheal Disease
71.5
Upper Respiratory Infection
2.9
Lower Respiratory Infection
103
Per this workshop on Group A Strep, an accelerated vaccine development schedule for a disease might typically take about eight years with a further eight years for global deployment. It estimates a more traditional development process at 13 years and deployment at 15-20 years thereafter.
If GiveWell charities buy a DALY at $80, it would be worth it to invest (for example) $3.2 billion to eliminate a single year of tuberculosis disease burden.
Good Solutions: While I have not done comprehensive research into potential strategies to deploy funds, there are several that are promising. I’ll make the case for two (advanced market commitments and challenge trials) below and briefly mention two more (systems immunology research and mRNA vaccine production subsidies).
An Advanced Market Commitment (AMC) involves committing ahead of time to purchase a significant number of effective vaccinations at a fairly high price. This (1) creates a greater profit incentive for developing vaccines; (2) reduces risks to pharma companies of being pressured to drastically reduce prices or give up IP once they’ve been authorized to sell an effective vaccine; and (3) generates funding to actually purchase and distribute vaccines, hopefully accelerating deployment and increasing manufacturing scale.
Operation Warp Speed is the most well-known example of an AMC and was one reason for the extremely rapid development of COVID vaccines. A previous $1.5 billion AMC for pneumooccus vaccines is estimated to have averted 570 thousand future deaths as of 2019 by accelerating vaccine administration. One analysis in 2005 found that an AMC for malaria of $3.1 billion ($4.3B in 2021 dollars) would cost less than $15 per DALY saved ($21 in 2021 dollars). To give a sense of plausibility and scale, a 2004 study found that every dollar of annual expected revenue for a vaccine yields 6 cents in annual R&D spending.
Challenge Studies: 1Day Sooner is best known for our advocacy of challenge studies, which are arguably a critical path for vaccine development in hepatitis c, tuberculosis, malaria, and group A strep. A challenge study can generate a preliminary estimate of vaccine efficacy for $5-10 million in six months where a traditional Phase 2B might cost $100 million over multiple years. For example, a recent paper this year published negative efficacy results for a promising hepatitis c candidate in a study of intravenous drug users that ran from 2013-2019. A challenge model could have generated that same answer in a fraction of the time, freeing resources to test new candidates (which is why leading hep c researchers have recently advocated for development of a challenge model). Scaling up challenge models to quickly test multiple vaccine candidates against each of the major infectious diseases and openly share results could usefully absorb hundreds of millions of dollars in fairly short order.
Basic Systems Immunology Research to use new technologies (like next generation sequencing and machine learning) to better understand and predict the immune response could also enhance the vaccine development process (by for example validating animal models of disease or developing an algorithmic model of the human immune response in which to test vaccines). And Subsidizing mRNA Vaccine Production Facilities could make it cheaper, easier, and faster to produce and deploy vaccines against a variety of diseases.
Good Timing:The extraordinarily rapid and successful development of COVID vaccines has proved faster development to be possible, validated multiple promising techniques, and brought unprecedented resources to the field. Promising developments in malaria vaccines have also emerged, and attention for pandemic preparedness and vaccine equity is also unusually high.
This momentum creates a chance to make the temporarily greater resources for vaccinology more permanent by attracting additional government and philanthropic funding first generated by COVID. A large public push of increased resources is more likely to be successful now and lead to a permanent shift in prioritization and capabilities than it has in the past or will in the future.
It’s important to note that different vaccine acceleration strategies are complementary: stimulating economic demand through AMCs makes pharma companies more interested in commercializing the vaccine candidates tested by challenge studies. An influx of funding can change expectations around development timing in a virtuous cycle (e.g. a pharma company assuming potential competitors will move more quickly by using challenge studies will itself move more quickly), which can itself attract more private and public funding. Additionally, improving deployment mechanisms relevant to any given vaccine may have a positive effect on deployment machinery for other vaccines as well.
Good for EA: Besides its direct benefits, investing in vaccine development helps achieve several EA goals.
Diversification: Investing in vaccine development provides useful diversification from other EA strategies. Diversification in philanthropy has a broadly similar logic as it does in finance: the future is uncertain; making bets that are uncorrelated with each other reduces the risk that a small set of miscalculations will tank all your returns. (Alexander Berger’s discussion of Open Phil’s worldview diversification here and Holden Karnofsky’s here may also have some relevance to this point). EAs invest in global health directly through GiveWell charity, in better policy outcomes through advocacy, and in existential risk through AI safety and pandemic preparedness. Addressing global health through vaccine development (via direct funding and advocacy) will be fairly uncorrelated from each of those approaches.
EA Reputation: Being identified with saving millions of lives through a highly salient campaign of rapid vaccine development will improve the EA brand, attract new members not otherwise interested in the EA movement, build EA equity in the pharma industry, and yield political gains that can be harvested to influence AI policy and other important areas. The EA movement being seen as owning an era of rapid vaccine success through high levels of donation has reputational benefits largely absent from GiveWell top charities (which ameliorate ongoing problems rather than creating highly salient solutions), AI risk reduction (benefits are uncertain, materialize in the long-term, and are hard to verify), or US advocacy areas (which are politically contentious).
Catastrophic Risk: Improving vaccine development in the medium term will help mitigate pandemic risk in the long-term by improving our scientific understanding and technological abilities and by creating a sustainable source of funding for the vaccinology, immunology, and infectious disease fields that will be crucial to addressing the next pandemic. Additionally, accruing equity in vaccine development will help EAs guide decision-making for pandemic preparedness policy more broadly by giving the EA movement a leadership role in the institutions that are making those decisions.
Good Arguments Against: Here are some weaknesses and possible arguments against the claims of this post:
No Rigorous Methodology: It is easy to use large numbers to make a potential cause area seem attractive, but achieving actual gains may be much more difficult than broad estimates might imply. For example, the AMC modeling literature cited here is mostly old, developed by AMC advocates, and lacks methodological rigor (and some of it seems to imply a relatively small impact).
Long-Term Disease Burden Could Be Much Lower: It will likely take at least a decade or more to deploy vaccines in the pipeline today, and then the period over which disease burden will be reduced will often be further decades in the future. To use one example, Group A Strep’s disease burden is largely due to deaths caused by rheumatic heart disease, which normally takes decades after initial infection to be lethal. Thus global economic development (particularly if significantly accelerated by general artificial intelligence) may significantly reduce the actual disease burden averted a significant period of time in the future.
1Day Sooner May Have Been Wrong about Covid Challenge: COVID challenge studies have not been meaningfully helpful to the current pandemic. This may imply 1Day Sooner’s judgment is poor (and/or that our ability to be persuasive may exceed our ability to be right).
Vaccines May Be Very Difficult to Develop: COVID was an unusually easy disease to vaccinate against because its main advantage is to spread quickly, and our immune response is quite effective to reinfection. By contrast diseases like tuberculosis or hepatitis c may be much more difficult to develop vaccines against (which is partly why the diseases available to target have resisted vaccine development for a century or so). HIV has had enormous resources put into vaccine development without much success. The malaria vaccine currently being deployed (which is only 30% effective) was initially tested in the 1980s, implying the level of resources described may not help make much progress, particularly when spread over long periods of time.
Vaccines Aren’t a Silver Bullet: A typhoid vaccine exists, but disease burden is still very significant. Vaccines can fail to be long-lasting or effective enough to be a cost-effective solution to effectively end disease burden ad may require significant ongoing use of resources to have an effect, reducing the cost-effectiveness of money spent on development and deployment.
Gates and Wellcome Already Fund This: Two of the world’s four largest foundations devote significant resources to vaccine development and deployment, which could indicate that the area is already well-funded.
Next Steps : I think the claims of this post are plausible and deserve significant investigation (and public explanation) from the EA community. This could be an excellent opportunity to save millions of lives cost-effectively while also helping to solve the “funding overhang” problem that may disincentivize EA from expanding and improving the EA brand to boot.
I don’t in any way claim my arguments above are ironclad or foolproof, but I think vaccine development deserves great consideration by the EA community and that learning to evaluate it publicly as an EA cause area can serve as a positive model for growth in other EA-potential projects.

I work at Open Philanthropy on cause prioritisation and on our science giving, and I agree with the direction of your conclusion here from a “Global Health and Wellbeing” point of view (i.e. rather than a longtermist POV), that funding particular infectious disease R&D could be as or more cost-effective at averting DALYs as GiveWell top charities. Indeed I’d expand what you’re saying from vaccines to other global health R&D - new therapeutics, new low cost diagnostics, new mosquito control tools, etc.
I’m not sure what level of investment that might remain true at, and we’re always interested to explore which diseases and health technologies might be most worth investing in. If you (Josh) or anyone else reading this has more ideas on what directions to head, or are interested in global health R&D and just want to say hi, feel free to comment here or email me at jacob [at] openphilanthropy [dot] org.
(For other readers, I know Josh via his work at 1Day Sooner, and we fund 1DS, but I didn’t know he was going to write this post, and stumbled on it organically. I liked it, thanks for writing it Josh!)