Total costs saved (direct + indirect) through sexual and reproductive healthcare is sourced from the Copenhagen Consensus, as their analysis indicates that for each dollar spent on SRHR, $120 would be saved.
I suppose the other numbers are extrapolations from this figure, though it's hard to say.
These cost effectiveness numbers are based on the total costs of our Outreach and Public Sector Strengthening programs in Nigeria and our impact based on services delivered through these channels and calculated using our Impact 2 tool. Costs include all actual expenses to MSI involved in delivering services through these two channels, for example, for our outreach teams, these costs encompass service and non service providers, consumables, travel, demand generation, quality assurance, and other overhead expenses associated with providing services on-site (such as Research, Monitoring and Evaluation). This also includes MSI's indirect costs.
For impact estimates, such as the number of maternal deaths averted, we utilize our Impact 2. This is an open-source, peer-reviewed tool that models bottom up estimates based on the services our teams deliver on the ground. The modelling is based on best available data from reputable sources such as WHO, UN, World Bank etc.
I'll be honest, to me the numbers sound too good to be true, so I'm curious to understand the assumptions that go into those numbers and whether I agree with them.
If the numbers really are that good that's quite exciting!
(The following is mostly copied from this thread due to a lack of time. I unfortunately can't commit to much engagement on replies to this.)
The sign of the effect of MSI seems to rely crucially on a very high credence in the person-affecting view, where the interests of future people are not considered.
Since 2000, MSI has averted one maternal death by preventing on average 502 unintended pregnancies. Even if only ~20% of these unintended pregnancies would have counterfactually been carried to term (due to abortion, replacement, and other factors), that still means preventing one maternal death prevents the creation of ~100 human beings. In other words, MSI's intervention prevents ~100x as much human life experience as it creates by averting a maternal death. If one desires to maximize expected choice-worthiness under moral uncertainty, assuming the value of human experience is independent of the person-affecting view, one must be ~99% confident that the person-affecting view is true for MSI to be net positive.
However, many EAs, especially longtermists, argue that the person-affecting view is unlikely to be true. For example, Will MacAskill spends most of Chapter 8 of What We Owe The Future arguing that "all proposed defences of the intuition of neutrality [i.e. person-affecting view] suffer from devastating objections". Toby Ord writes in The Precipice p. 263 that "Any plausible account of population ethics will involve…making sacrifices on behalf of merely possible people."
If there's a significant probability that the person-affecting view may be false, then MSI's effect could in reality be up to 100x as negative as its effect on mothers is positive.
There is also a mental health benefit to averting unwanted pregnancy. A meta-analysis by Wang et al. (2021)found that women with an unplanned pregnancy were 62% more likely (28% vs. 17%) to suffer postpartum depression compared to women with a planned pregnancy. We don't have good data on depression prevalence among women whose unplanned pregnancy was averted, but it seems probable that an unplanned pregnancy increases the risk of mental illness, even if only by adding another life stressor. It is very hard to measure, but I suspect that the wellbeing benefits of not having one's education cut short / career & income disrupted / living with stigma of being a single mother or with a partner you didn't choose to have a child with / etc. are high.
For us, high-impact clients include adolescents (under the age of 20), individuals living in multi-dimensional poverty, those who aren’t using or have never used contraception, and those who have no other options for the services we provide. Collectively, we aim for over 80% of our clients to be from one or more of these high-impact groups.
I think this is a good way of trying to secure strong counterfactual impact. I notice that your cost-effectiveness estimates imply that you prevent 200 maternal deaths per 100,000 averted pregnancies. How do you arrive at this figure, given the lack of maternal mortality data for your specific demographic (unwanted pregnancy, rural, underserved, low-income country)? Nigeria has the 2nd-worst maternal mortality rate in the world, at 112 per 100,000 - but your Nigeria numbers suggest something like 500 per 100,000.
Another interesting thing is that you avert a maternal death for $3,353 - which means maybe $70-100 per extra year of life that these women get - and you avert a DALY for $4.77. This implies that averted maternal deaths only account for ~5% of the health benefits you are measuring. Where are the other 95% coming from? Importantly, are any coming from the infant or from non-health benefits converted into DALYs - because counting these would be moral assumptions worth flagging.
Thank you so much for your thoughtful comment and for sharing the research on post-partum depression which we look forward to reviewing. Thanks also for your questions about DALYs and maternal deaths averted. We will provide more information shortly!
An excellent writeup - thank you to the MSI team for taking the time as a large existing global health/development org to share this. I'm particularly excited to see the potential cost-effectiveness of last mile programming where the benefits to reproductive autonomy are likely to be particularly strong.
Executive summary: MSI Reproductive Choices has served over 200 million clients since 1976, delivering highly cost-effective sexual and reproductive healthcare services focused on underserved communities in Africa, Asia, and Latin America.
Key points:
MSI's services have averted an estimated 316,000 maternal deaths and 158.6 million unintended pregnancies since 2000, at an average cost of $4.70 per DALY and $3,353 per maternal death averted globally.
MSI reaches last-mile communities through mobile outreach teams, partnerships with public sector facilities, and a network of local midwives and nurses called MSI Ladies.
In 2023, MSI served 23.3 million clients, with 57% having no other service options, 31% living in multi-dimensional poverty, and 19% being adolescents.
MSI's services in 2023 are estimated to save 37,500 lives, prevent 16.5 million unintended pregnancies, avert 9 million unsafe abortions, and save $11.2 million in direct healthcare costs for low- and middle-income countries.
MSI Nigeria, the most cost-effective program, has a cost per DALY of $1.63 and per maternal death averted of $685, with significant potential for expansion to meet the country's high unmet need for contraception.
This comment was auto-generated by the EA Forum Team. Feel free to point out issues with this summary by replying to the comment, and contact us if you have feedback.
BLUF:
* To determine whether AI is ‘improving exponentially’, ‘hitting the wall’, or any other claim which involves a quantity or magnitude (e.g. ‘This model was a big leap/small increment’). We need a good y-axis: an interval scale of AI capability which means +1 unit always represents the same degree of ‘how much better’, in the same way +1 degree Celsius is always the same amount of ‘how much hotter’.
* Yet there is no good y-axis for AI capability. All our...
Summary
* The animal welfare movement has already seen an influx in funding and should prepare for the possibility of more.
* The EA Animal Welfare Fund is encouraging those working in animal advocacy to actively set aside time and resources now to concretely plan for scaling sustainably, and we’ll support you in doing that.
* We’re requesting advocates set concrete ambitious goals and submit plans t...
Public service announcement
1. Applications are now open for our first ever round of the Charity Entrepreneurship Incubation Program dedicated exclusively to animal welfare. Learn more about what’s different this round here and apply...
In 1976, our founder Tim Black established MSI Reproductive Choices[1] to bring contraception and abortion care to women in underserved communities that no one else would go to. As a doctor, he witnessed firsthand the hardship caused by the lack of reproductive choice and accordingly, he established quality care, cost-effectiveness, data, and sustainability as foundational principles of the organization. Nearly 50 years later, this legacy remains at the core of MSI Reproductive Choices today.
Since our founding, MSI has served more than 200 million clients, of which more than 100 million were served in the last nine years. Since 2000, our global services have averted an estimated 316,000 maternal deaths and 158.6 million unintended pregnancies.
We deliver impact with exceptional cost-effectiveness. On a global scale via our Outreach and Public Sector Strengthening programs, which reach underserved “last mile” communities, our average cost per disability-adjusted life year (DALY) is $4.70[2], and our average cost per maternal death averted is $3,353. In Nigeria, our most cost-effective program, these figures drop to just $1.63 per DALY and $685 per maternal death averted in our programming with the most underserved communities.[3]
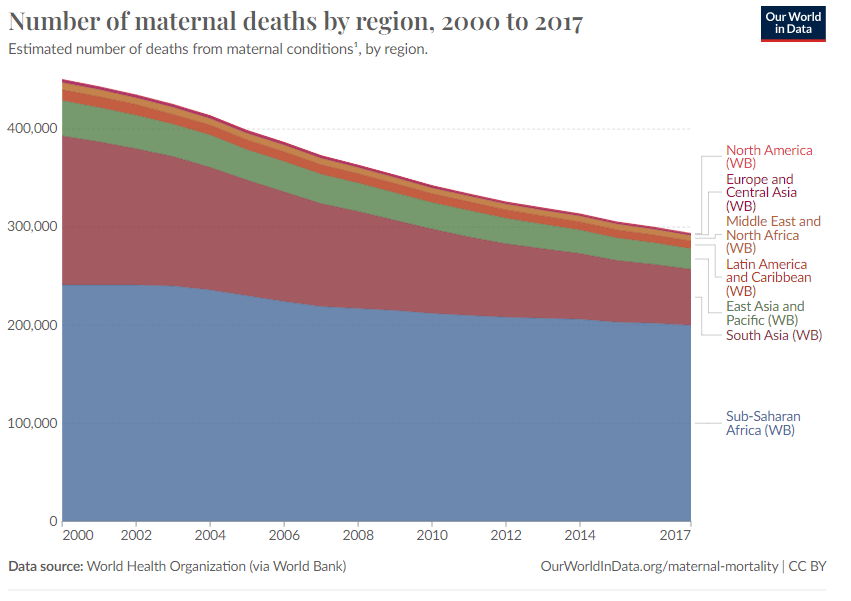
The global disparity between the rate of maternal deaths is evident in low-income countries. In 2020, the Maternal Mortality Ratio (MMR) reached 430 per 100,000 live births in low-income countries, a significant contrast to just 12 per 100,000 live births in high-income nations. In some countries, like Nigeria, the maternal mortality rate exceeds 1,000 per 100,000 live births.
Demand for family planning and sexual and reproductive healthcare services will continue to grow, and by 2030, an additional 180 million women will need access to these services. The urgency of this need is emphasized by theadolescent girls in low- and middle-income countries who wish to avoid pregnancy, yet a significant 43% of them face an unmet need for contraception. Pregnancy-related deaths are the leading cause of death for adolescent girls globally.
The World Health Organization has stressed that to avoid maternal deaths, it is vital to prevent unintended pregnancies. They stated: “all women, including adolescents, need access to contraception, safe abortion services to the full extent of the law, and quality post-abortion care.”
Gender Equality and Empowerment: Family planning empowers individuals, especially women, to make informed choices about their reproductive health. When people have access to contraception and family planning services, they have greater control over their bodies and lives, leading to improved well-being and autonomy. Access to contraceptive information is central to achieving gender equality. When women and couples are empowered to plan if and when to have children, as well as how many, women are more likely to complete their education. Their autonomy within households increases, and their earning potential improves. This strengthens their economic security and well-being, along with that of their families.
Poverty Reduction: By preventing unintended pregnancies, family planning helps families manage their resources more effectively. When parents can plan the size of their families, they are better able to provide for their children's needs, breaking the cycle of poverty. Cumulatively, these benefits contribute to poverty reduction and global development.
Where We Work and How We Work
MSI operates in 36 countries across 6 continents with a dedicated team of 9,000 members. Our global support offices are in the United States, the United Kingdom, and Australia. Our country programs that deliver sexual and reproductive health services are primarily located in Africa, Asia, and Latin America. A complete list of countries where we work can be found here.
At MSI, our mission is to maximize impact while ensuring quality, client-centered care that offers excellent value for money for funders. In 2023, we served 23.3 million clients, marking a tenfold increase since 2000. Our ability to deliver services at scale has significantly boosted modern contraceptive prevalence rates (mCPR) in the regions we serve. For instance, in Senegal, we have played a key role in increasing mCPR from 8% in 2010 to over 20% by 2022, contributing approximately 40% to this growth. This achievement is largely due to our efforts in scaling up services, reaching new users, and expanding access to family planning methods, particularly long-acting reversible contraceptives (LARCs).
Our Solutions: We reach 30,000+ communities globally each year through direct service delivery and partnerships with the public and private sectors. Our models include:
300+ mobile outreach teams: Outreach is our most effective way of reaching the millions who lack access to contraception, particularly in rural communities; 57% of the people we serve have no other options for getting the contraceptive service they receive from our outreach team. Our 360° outreach teams will drive, fly, sail, or trek to deliver services to remote and rural communities. In 2023, these teams served over 4 million clients.
6,000+ public sector facilities: Our long-standing partnership with the public sector leverages existing public resources and builds capacity via training, quality assurance, and supportive supervision to ensure public sector clients have access to high-quality family planning services. This solution is strategically designed with the ultimate objective of full handover of all quality assurance and support activities to the government, ensuring sustained, long-term impact. We estimate to have trained 12,000 public sector providers across these 6,000 sites and, in 2023, these facilities served over 7 million clients.
750 MSI Ladies: MSI Ladies, often local midwives and nurses, offer discreet, accessible, and affordable services to women and girls in their communities. They usually work from their home, their clinic, or pharmacies, or can visit clients in their own homes. In 2023, these MSI Ladies served over 885,000 clients.
These three models described above form our strategy for reaching last-mile communities and ensuring no one is left behind. These models are highly cost-effective and deliver at scale. Additionally, we expand access through centers and maternities, product sales which we call social marketing and a network of private providers. Learn more about our programs here.
Our Clients and Impact
Our teams go to the last mile, beyond the reach of public health systems to serve those who have the highest need and the fewest options. We focus on what we call high-impact clients, because reaching them will have the greatest impact and create the most significant change. For us, high-impact clients include adolescents (under the age of 20), individuals living in multi-dimensional poverty, those who aren’t using or have never used contraception, and those who have no other options for the services we provide. Collectively, we aim for over 80% of our clients to be from one or more of these high-impact groups. We arecurrently successfully increasing our reach in each of these high-impact groups through our last mile programming:
57% of our clients knew of no other option for their service.
31% of our clients were living in multi-dimensional poverty.
19% of our clients are adolescents. In just six years, we have almost tripled adolescent reach across our country programs from 6% to 19%, meaning one in six of our clients are adolescents. [4]
33% of our clients are first-time users of contraception and 58% are adopters, meaning they weren’t using modern contraception before receiving services.
MSI estimates that the services we delivered in 2023 will have the following impact[5]:
37,500 women and girls' lives saved.
16.5 million unintended pregnancies prevented.
9 million unsafe abortions averted.
23 million DALYs averted.
$11.2 million saved for low- and middle-income countries in direct healthcare costs.
35.4 million contraceptive couple years of protection (CYP) generated*.
13 policy, legal, or regulatory changes influenced by our advocacy efforts.
We estimate that, on average, over 20% of the demand for family planning in the countries where we operate was met by MSI-supported services in 2023. In some countries, such as Sierra Leone and Tanzania, this percentage exceeds 40%. Read more about MSI’s impact here.
We developed a peer-reviewed, sector-renowned tool for measuring impactbeyond methods provided called Impact2. This was the first reproductive health model based on service provision data, enabling users to estimate the wider health, demographic, and economic impacts of family planning and safe abortion services. Peer reviewed and published in the British Medical Journal, Impact 2 leads the sector, with thousands of downloads made every year by governments, researchers, implementing partners, and donors alike. Learn more about the methodology behind calculating impact, such as maternal deaths averted, here.
We have also recently developed the Impact Investment tool to help donors calculate the impact of a donation to MSI, here.
Monitoring and Evaluation
MSI is data-driven and evidence-based, and we are recognized throughout the sector and beyond for our exceptional focus on data. Through the utilization of a diverse array of data sources, ranging from routine client data to client exit interviews, feedback mechanisms, aligned financial systems, and geolocation data, our organization has cultivated a robust monitoring and evaluation framework. This wealth of data enables us to track, monitor, and better understand performance in real-time, enabling swift course corrections for our country programs. Annually, we process over 300 million data points from our clients, offering invaluable insights into their demographics, service preferences, and utilization patterns.
Our Client Exit Interviews (CEI), conducted annually as a representative survey of clients across our partnership, have provided invaluable insights since 2011. Having heard the voices of over 200,000 clients, this initiative enhances our understanding by exploring the decision-making processes involved in service uptake, method selection, and the quality of care experienced by our clients.
The cornerstone of our success lies in our integrated data system, featuring unique team cost identifiers and interactive dashboards used by our operational teams on a daily basis. This infrastructure allows for the rapid dissemination of insights across our partnership, fostering cross-fertilization of ideas and nimble adaptation strategies. Our harmonized financial system enables transparent tracking of expenditure from its source to the community it serves, facilitating the quantification of outcomes in terms of the population reached and services delivered.
In tandem with the power of this data, we foster collaborations with esteemed research institutions such as John Hopkins, Population Council, and the Guttmacher Institute, and many others to tackle complex questions regarding the broader impact of our initiatives.
The culmination of these efforts empowers MSI to not only monitor and evaluate program performance comprehensively but also to optimize resource allocation, identify cost inefficiencies, and enact agile responses to evolving challenges. By harnessing the full potential of data-driven insights and fostering a culture of collaboration and adaptability, we remain steadfast in our commitment to advancing reproductive health outcomes worldwide.
Cost-Effectiveness
MSI is a highly cost-effective organization, and focusing on cost-effectiveness is part of our DNA because we know that every dollar could be spent improving or saving lives.
Costs vary by country based on context, mix of service delivery channels, and scale. Globally, the average costs across our Outreach and Public Sector Strengthening “last mile” channels are:
Cost per client reached: $10.26
Cost per unintended pregnancies averted: $8.16
Cost per maternal death averted: $3,353
Cost per DALY averted: $4.70
Costs per couple years of protection (CYP): $4.88
When looking at our Outreach and Public sector strengthening channels, Nigeria, Sierra Leone, the DRC, Tanzania, and Uganda were among our five most cost-effective countries. The services delivered in 2023 will have the following estimated impact:
Our Most Cost-Effective Program: An Overview of MSI Nigeria
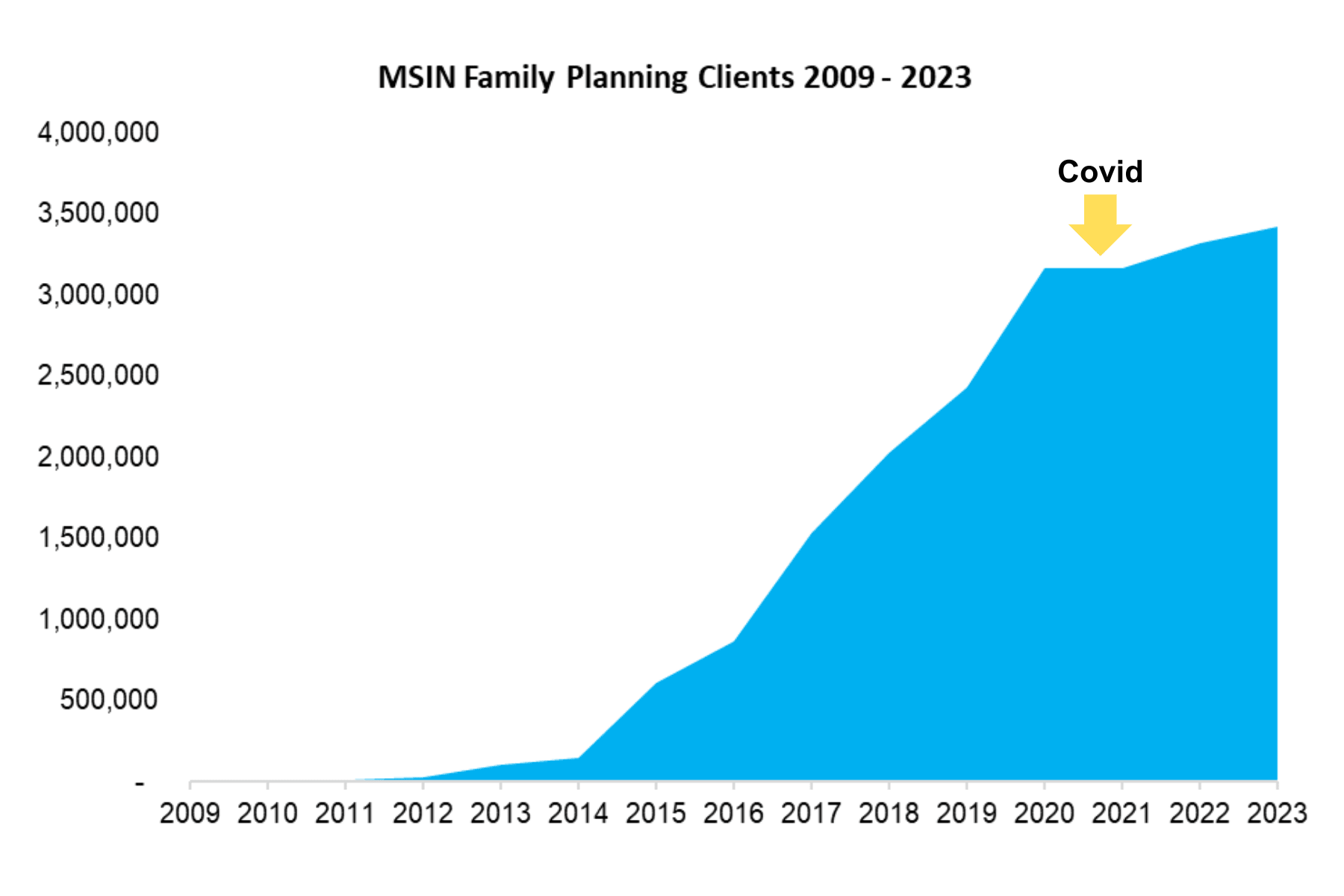
Founded in 2009, MSI Nigeria (MSIN) has a remarkable story of growth. It is now the leading sexual and reproductive healthcare provider in the country. MSIN’s last mile programming is centered around its 24 mobile outreach teams and its support of 2,700 public health facilities.MSIN stands as the largest trainer of public providers in the country and has served more than21 million people to date.
Since its inception, MSIN has significantly increased the number of family planning services it delivers directly through Outreach teams and in partnership with the public sector. This growth is evident in the chart below:
In 2023, MSIN's efforts through outreach and public sector strengthening served nearly 3.2 million clients, providing them with access to the services of their choice. This has led to significant impacts, as outlined below:
4.1 million unintended pregnancies prevented.
9 million DALYs averted.
21,587 maternal deaths adverted.
6.4 million CYPs generated.
MSIN has done exceptionally well in reaching high-impact clients through its last mile programming:
64% knew of no other option for their service.
73% are adopters of contraception, and 39% were first-time users.
32% are under the age of 20.
MSIN is able to deliver high-quality, client-centered care through outreach and public sector strengthening with extraordinary cost-effectiveness:
Cost per client served: $4.7
Cost per unintended pregnancies averted: $3.60
Cost per maternal death averted: $685
Cost per DALY: $1.63
Cost per CYP: $2.31
What’s next in Nigeria?
Despite the progress made, Nigeria still has at least 14.5 million people who want access to contraception but cannot obtain it, and this figure continues to grow as demand rises. MSIN has a big vision for 2030: to support at least 20% of Nigeria’s 28,000 public sector sites, double mCPR, make contraception access a reality across the country while continuing to fill immediate gaps in the health system through outreach. There is significant room for the program to expand, and MSIN is well-positioned to utilize additional investment to fulfill this vision.
Where else could your support make a difference?
All of our country programs have additional scope for investment and absorption of funds. Our models are documented, replicable, and scalable.
In addition to the other most cost-effective programs (Nigeria, Sierra Leone, Tanzania, and Uganda), the Democratic Republic of Congo (DRC) stands out as a country where further investment could have a significant impact. Launched in 2018, the DRC is our newest program and currently has a cost per CYP of $9.54- a 64% decrease since 2019. At this rate, we estimate that within 2 -3 years, the DRC program could achieve similar cost-effectiveness to Nigeria, and the program will reach a million people in the next 3 years.
Like Nigeria, DRC has one of the world’s lowest contraceptive prevalence rates, around 15%. In many of the communities we work in, this rate is 1% or less when we first begin providing services.
Want to hear more?
MSI will be attending the EA Global Conference in London in May 2024. Whether you're curious about our models, interested in collaborating, or simply want to learn more about our data and cost-effectiveness, please reach out to us through the conference platform if you would like to connect.
If you and/or your organization are interested in hearing more about our sector-leading evidence and impact calculators, MSI’s Evidence and Impact team host regular webinars on the latest advancements of our Impact tools. Please reach out at [email protected].
If you would like to donate today towards data-backed impactful programs for reproductive choice worldwide, please visit our website here if you are outside of the US or here if you want to donate to our US 501c3. You can also contact us at [email protected]for more information on ways to support our work.
[2]All figures in this post are in United States Dollars (USD).
[3]Please note that our Outreach channel costs include 100% of costs as it is entirely delivered by MSI. For our Public Sector Strengthening (PSS) channel, cost-effectiveness is calculated based on MSI’s direct costs. We recognize that there are also costs incurred by the local health system, for example, provider salaries, that are not accounted for.
[4]The adolescent statistics are from our outreach program. The data from our public sector strengthening work is not yet available across all country programs.
[5]These results are all encompassing of MSI’s global partnership of country programs, across all channels using our Impact 2 tool.



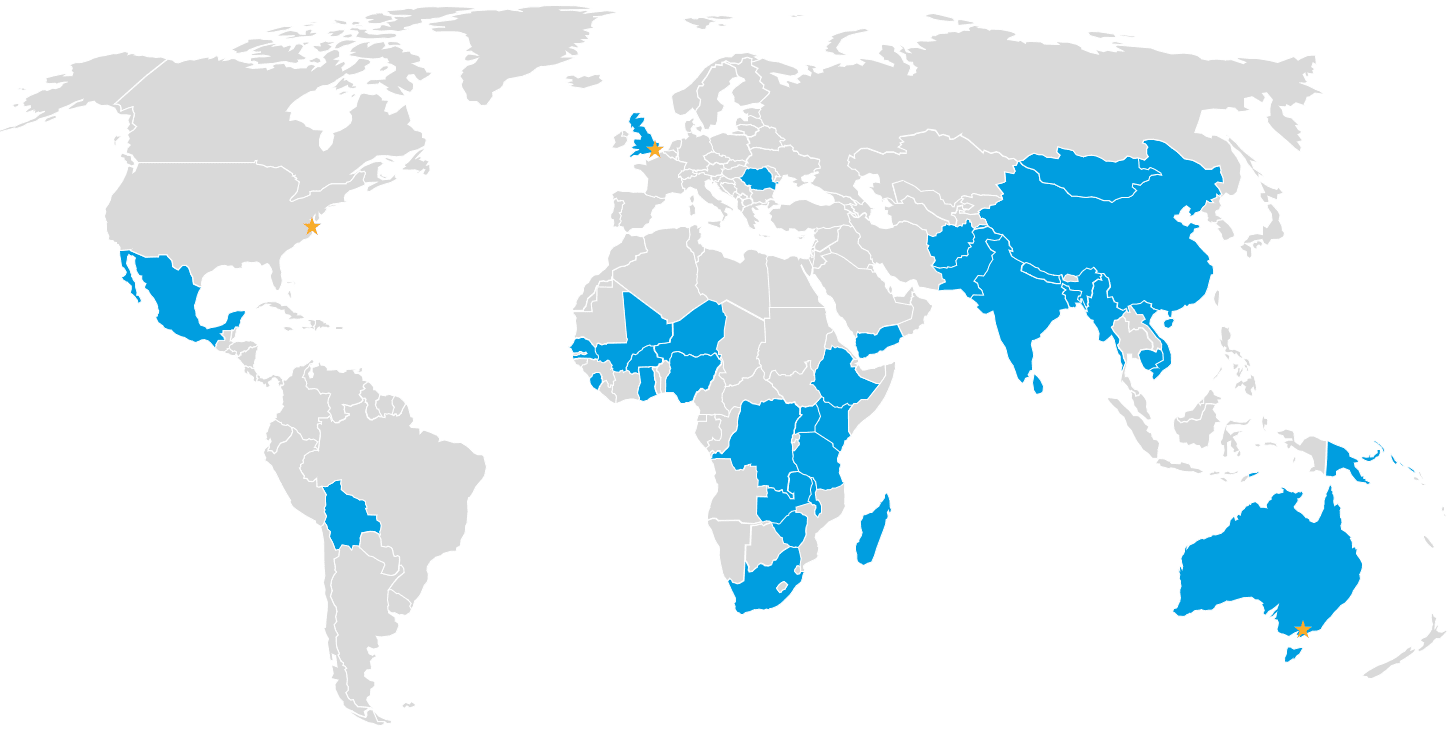 MSI operates in 36 countries across 6 continents with a dedicated team of 9,000 members. Our global support offices are in the United States, the United Kingdom, and Australia. Our country programs that deliver sexual and reproductive health services are primarily located in Africa, Asia, and Latin America. A complete list of countries where we work can be found
MSI operates in 36 countries across 6 continents with a dedicated team of 9,000 members. Our global support offices are in the United States, the United Kingdom, and Australia. Our country programs that deliver sexual and reproductive health services are primarily located in Africa, Asia, and Latin America. A complete list of countries where we work can be found 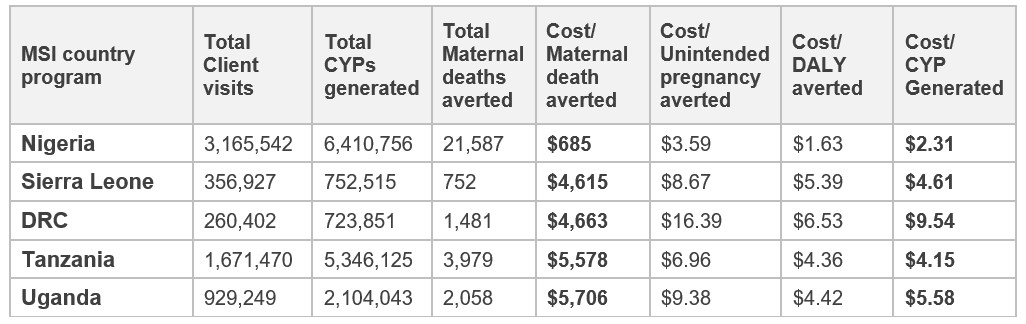
Is there a cost-effectiveness analysis available where I can read how you arrived at these numbers?
This note says:
I suppose the other numbers are extrapolations from this figure, though it's hard to say.
These cost effectiveness numbers are based on the total costs of our Outreach and Public Sector Strengthening programs in Nigeria and our impact based on services delivered through these channels and calculated using our Impact 2 tool. Costs include all actual expenses to MSI involved in delivering services through these two channels, for example, for our outreach teams, these costs encompass service and non service providers, consumables, travel, demand generation, quality assurance, and other overhead expenses associated with providing services on-site (such as Research, Monitoring and Evaluation). This also includes MSI's indirect costs.
For impact estimates, such as the number of maternal deaths averted, we utilize our Impact 2. This is an open-source, peer-reviewed tool that models bottom up estimates based on the services our teams deliver on the ground. The modelling is based on best available data from reputable sources such as WHO, UN, World Bank etc.
You can read more about Impact 2 via this introductory guide here: https://www.msichoices.org/wp-content/uploads/2023/10/impact-2-introductory-guide-june-2018-1.pdf
The full methodology paper can be found here: https://www.msichoices.org/wp-content/uploads/2023/10/impact-26-methodology-paper-2023.pdf
You can download the tool here: https://www.msichoices.org/what-we-do/technical-expertise/impact-2/
We will be publishing a follow-up blog with a deep dive on our Nigerian program and its cost effectiveness calculations soon.
Thanks, I'm looking forward to that post!
I'll be honest, to me the numbers sound too good to be true, so I'm curious to understand the assumptions that go into those numbers and whether I agree with them.
If the numbers really are that good that's quite exciting!
Thanks so much, we will share more soon!