Comments
Hurray for Draft Amnesty Day.
Threads -
Akash [1] - Targeted Anemia Treatment
Akash [2] - Critique of Fortify Health and Iron Fortification in India
Brendan [1] - Response to Critique
GiveWell - Change Our Mind Contest Reflections
This was a WIP response to Brendan, co-founder of Fortify Health, who responded to my critique on iron fortification in India that was originally written for the GiveWell Change Our Mind contest. I had abandoned writing this upon realising the complex terrain I would have to traverse to get to somewhere meaningful. Happily, all is not lost as today is Draft Amnesty Day.
I am also quite chuffed that GiveWell deemed my entry useful and mentioned the line of reasoning I dig into as worth looking into -
Some entries covered ideas we hadn't considered but found worth pursuing. For example, an entry arguing that iron fortification might be less cost-effective than we think inspired us to dig into the questions it raised about the prevalence of iron deficiency anemia in India. In this case, our current best guess is that our view on iron fortification won't change much, but we believe it's worthwhile for us to consider this issue.
So it is in the modest hope that some of these trains of thought are worth onboarding that I present an attempt to iron out some iron matters -
When are different thresholds for what is healthy across populations acceptable?
- While I’m sympathetic to concerns about imposing inappropriate standards of “normal,” I am also wary of redefining the threshold for acceptable health on regional norms that could inappropriately accept a lower standard under false claims of biological difference. - Brendan
Being wary of imposing differing biological values based on race/ethnicity is important. However, we should also be wary of ignoring biological differences - they can exist for biologically valid evolutionary reasons. A relevant example is sickle cell anemia rates being higher in Saharan Africa.
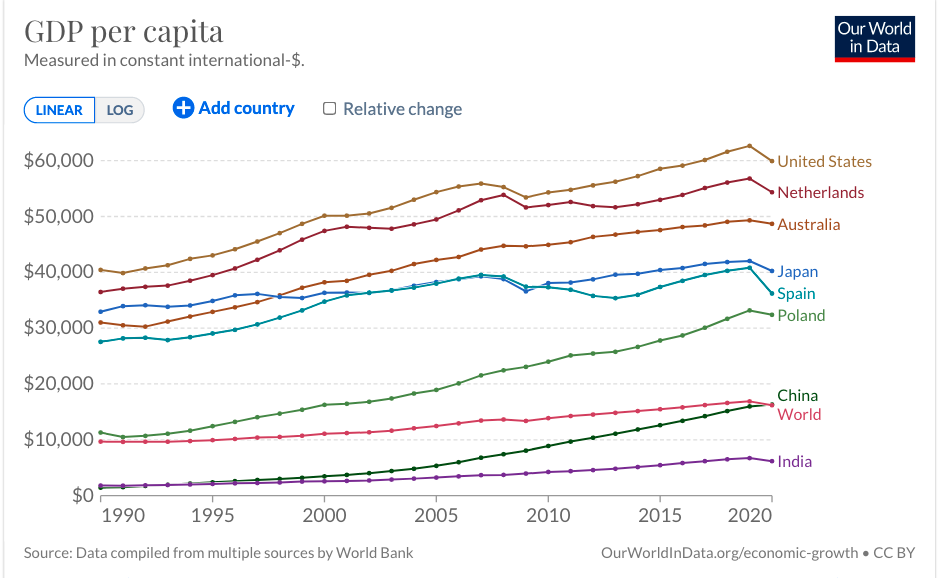
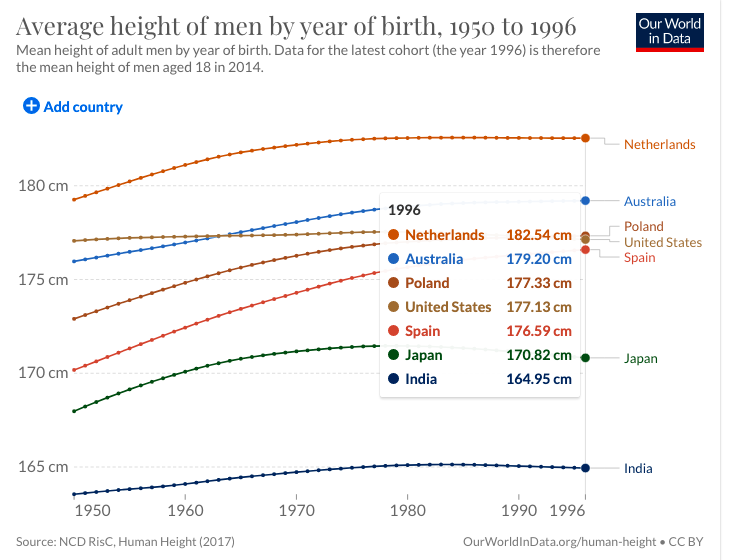
- The case of height is illustrative. Brendan rightly points out that stunting can be due to malnutrition and any claim that Indians are shorter than Americans should be treated with caution as societal reasons are causally related. However, we can also clearly see big differences in height across countries even when we roughly control for socioeconomic factors - for instance the height of men in Japan and Spain is significantly different even though the GDP per capita is similar.
Crucially the height/stunting example sheds light on the two sub-questions that interact when thinking of interventions meant to address differences in populations- 1. Is the difference biological vs societal and
2. Does the difference lead to, or is a proxy for, negative health outcomes?
- If differences are biological + have no health consequences, interventions to ‘fix’ these differences are misguided/unlikely to succeed (e.g. an intervention to increase the height of Japanese people). However, if differences are societal, there is good reason to implement interventions to negate these differences (stunting in Indian children). The answer to 1. interacts with the answer to 2. -> if a difference is due to societal factors it likely will lead/is a proxy for non-optimal well-being.
Iron-deficiency anemia and varying hemoglobin thresholds
When it comes to iron-deficiency anemia - the answer to 1. societal vs biological - appears to be hotly debated and underlies motivation to revise hemoglobin thresholds. It was the subject of a 2019 WHO stakeholder meeting as well as explored in subsequent papers such as Addo, 2021 and Sachdev 2021.
- This appears to remain an unsolved problem (from the WHO report) -
- Addressing ethnicity in the definition of anemia was proposed, as well as considerations about its role in influencing thresholds. It was observed that evidence for thresholds for infants and older persons was inadequate, that differences in thresholds between the sexes should be considered for all age groups, and that how genetic variation should be accounted for is an unresolved issue that clearly affects some settings more than others. It was emphasized that different settings may require distinct thresholds for anemia given the genetic variations associated with anemia.
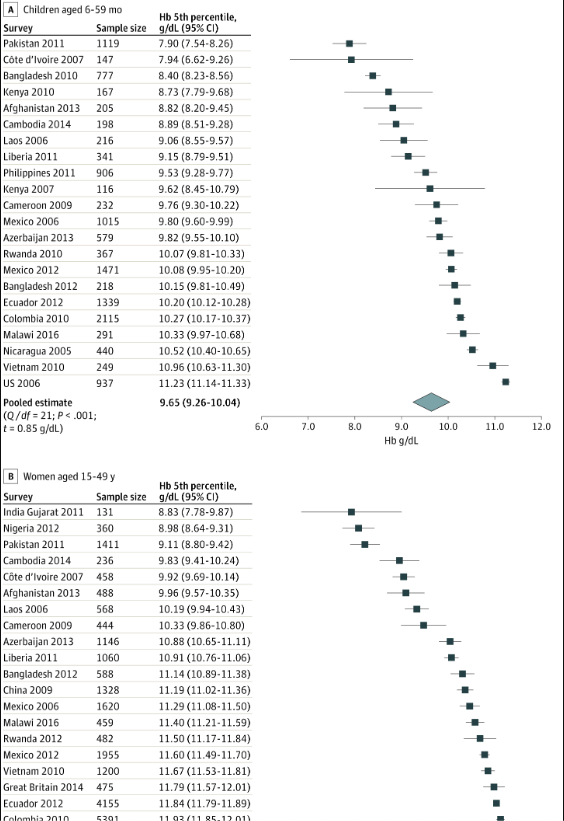
- Addo, 2021 asked whether hemoglobin thresholds differed amongst ‘healthy’ populations and analyzed data from 25 different countries, finding significant variation in these thresholds from those mandated by the WHO. The authors pooled Hb thresholds across studies and countries and arrived at “multinational estimates of Hb fifth percentile were 1.35 and 1.19 g/dL lower than the current WHO Hb cutoffs for defining anemia among preschool children and nonpregnant women”.
- Sachdev, 2021 focused specifically on Indian adolescents and used the distribution of hemoglobin in a healthy subpopulation to arrive at percentile-derived thresholds. Based on these thresholds, they argue that anemia prevalence among Indian adolescents is lower than generally estimated (and the same logic likely applies for Indian adults as I argue in posts 1. and 2.)
Do hemoglobin differences result from biological or societal factors?
A key question that Brendan raises and that applies to both these studies is - how do we know if a subpopulation is as healthy as they would be under ideal societal conditions? Both papers rely on criteria based on the absence of disease, inflammation and vitamin deficiencies, Brendan comments that “it is not clear [to me] that those who remain would not be healthier if they had higher hemoglobin levels”.
One way we could get at whether hemoglobin levels naturally vary in populations of healthy people is by looking at a multiethnic population.
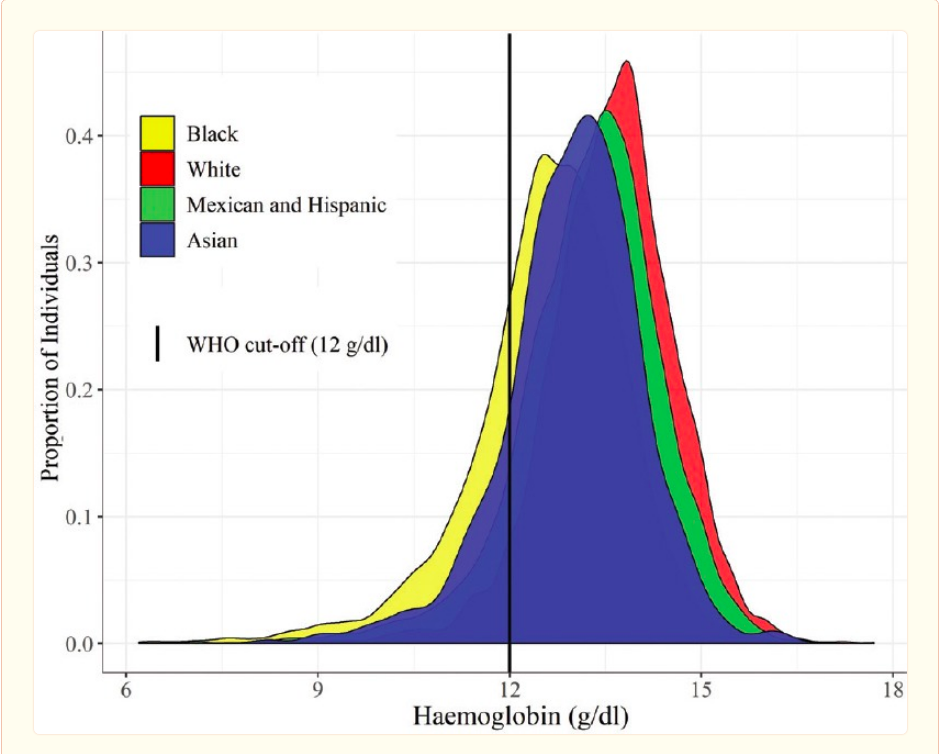
- For instance, it could be useful to look at hemoglobin levels amongst White and Asian populations in the United States. A Lim 2015 looked at reference intervals for various biochemical tests, including hemoglobin, amongst different ethnic groups - Whites, Asians, Hispanics, and Blacks - focusing on self-reported healthy individuals. They found that - “Compared to Whites, Asians have lower RIs in creatinine, hematocrit, hemoglobin, mean cell hemoglobin, MCHC, and mean platelet volume and higher normal ranges in globulin and total protein.”
- While the study did not control for socio-economic status (SES), it’s worth noting that Asians as a monolithic group have higher incomes than Whites, which can be used as a rough proxy for access to quality healthcare/nutrition that could skew results.
- Note that the broad ethnic characterization of ethnicities as well as the self-report nature of the study prevents any strong conclusions. In particular, as Brendan noted, meat-eating can be an important factor in hemoglobin levels, and it’s possible that the Asian group in the study was skewed towards vegetarianism/veganism. However, except for Indians (~30% of whom tend to be vegetarian), most Asians eat meat and Indian-Americans make up ~20% of Asians. Hence, the relative % increase in Asian participants who don’t eat meat is ~6% (n=480), which doesn’t seem big enough to impact the results, although isn’t out of the question.
- A similar study Varghese 2019 analyzed data from UK and US national surveys and found differing hemoglobin thresholds for women in different ethnic groups, with self-reported ‘healthy’ Asian women having lower hemoglobin values than White women. The authors suggest a couple of different reasons why this might be the case such as genetic and skeletal muscle mass variation.
- There is even evidence that hemoglobin levels can vary significantly in the same ethnic group in different geographic locations. Sala, 2008 found that “Normal subjects of different age groups from a northern Italian isolate have significantly higher hemoglobin levels when compared to matched subjects of southern Italian isolates”.
What if everyone is better off with higher hemoglobin levels, irrespective of the nature of the difference?
We still don’t know whether people are generally better off with higher hemoglobin levels. Suppose we take the above evidence to suggest that hemoglobin levels vary naturally in population subgroups, how does this relate to whether these differences lead to negative health benefits and should be corrected by interventions?
- Unlike the height example, where the outcome was a proxy of health (being stunted indicates severe malnutrition), hemoglobin levels are an outcome causally related to health (physically exertion, cognition, etc)
- Hence, even if variation is primarily caused by biological factors, there may be motivation to pursue interventions for their benefits. That is, Asian women may have lower hemoglobin levels due to genetic reasons but more hemoglobin, regardless of ethnicity, is preventative against maternal mortality
- In their review of ethnic influences on population reference values, Tahmahsebi 2018 makes the important point that differences may be due to ethnic-specific susceptibility to disease - “One important consideration is to determine whether these differences represent ethnic-specific susceptibility to diseases. While PSA, as an example, has been shown to be relatively higher in Blacks, Blacks have also been reported to have a higher prevalence of prostate cancer. Thus, it may be advisable to not treat higher levels of such biomarkers as healthy in certain ethnic groups.”
The map is the hemoglobin levels, the territory is the clinical and functional outcomes
Hemoglobin levels are useless in isolation, what we really care about is how people feel, behave and function.
Highly relevant graph from Addo, 2021 -
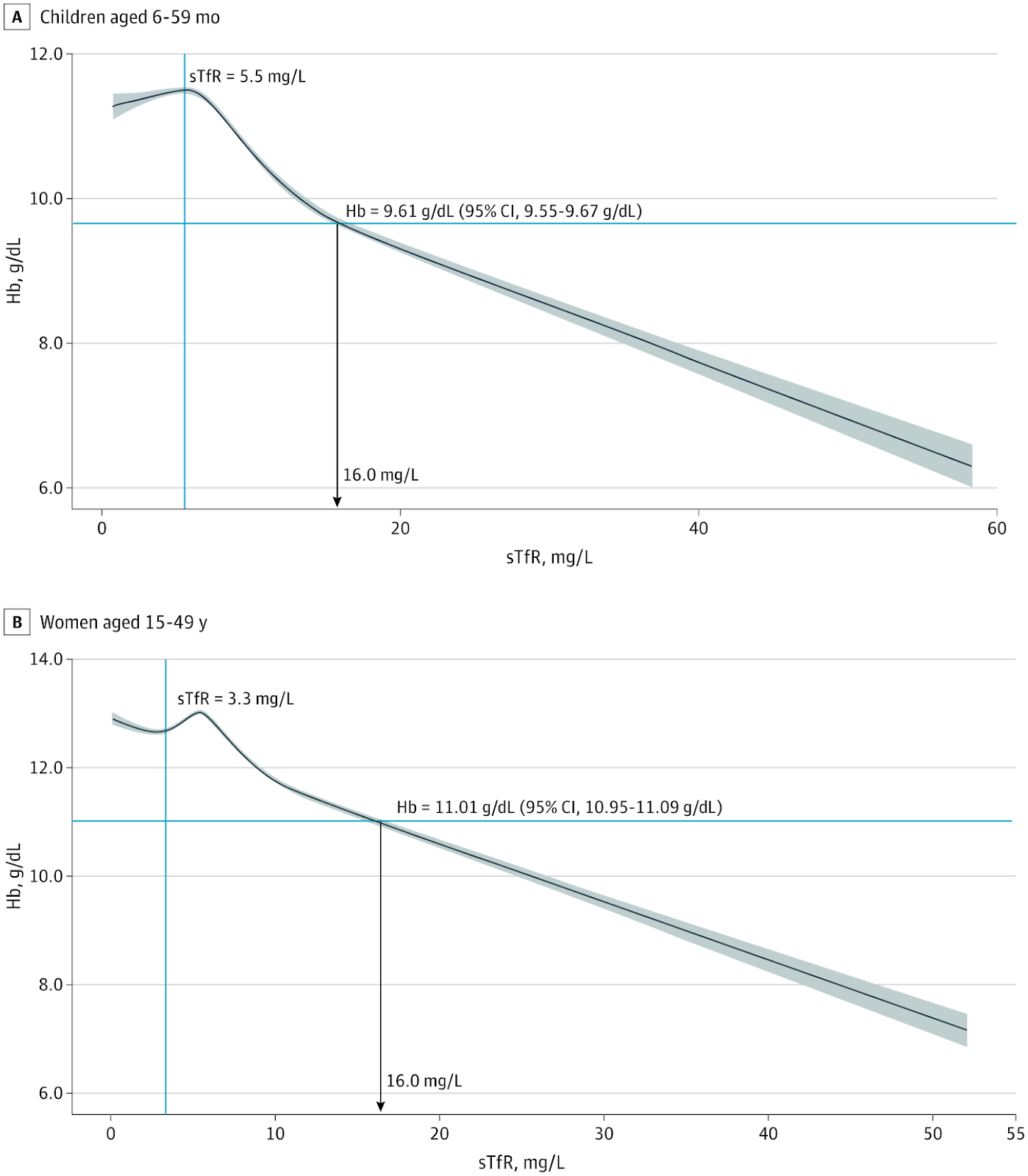
Where possible, Hb cutoffs defining anemia and its severity should be guided by functional and clinically relevant outcomes. Although clinical outcomes were not available in this work, we modeled Hb to sTfR concentrations, which physiologically reflect erythropoiesis. The curves of Hb-sTfR concentrations indicate distinct curvilinear and linear erythropoietic drive phases when Hb values are below a threshold (9.61 g/dL in children and 11.01 g/dL in women). The linear erythropoietic drive phase describes the expected compensatory physiological response to anemia, including increased tissue demand for iron and increased erythroid in the bone marrow. The physiological Hb-sTfR curves support the use of a pooled multinational Hb fifth percentile for defining anemia, as opposed to adopting Hb estimates that are specific to a survey, country, or race/ethnicity, which could lead to proliferation of multiple different Hb cutoffs and, thus, complicate their clinical application and global disease burden quantification, among other factors. We found that in both preschool children and women, regardless of Hb distribution, the population fifth percentile Hb was lower than 9.61 g/dL and 11.01 g/dL, indicating that tissue ID has already ensued The Hb fifth percentile derived in this analysis may reflect the development of anemia apparently caused by ID.
Re-evaluating past studies in light of new thresholds
In a conversation I had with Brendan, he pointed out an interesting point I'd missed. New thresholds that decrease the actual prevalence of anemia in a region can also increase the impact of iron interventions as it implies benefits seen in previous studies were large enough to persist despite the inclusion of 'non-target' participants.
It might be possible to re-evaluate some previous studies using the Hb to sTfR curve.
Appreciation for EA
I'm glad that Open Philanthropy and Givewell launched contests that incentivised me to do deep dives and write down my thoughts, that the culture of the Forum and the community is such that criticisms from random strangers are taken seriously and engaged with, and for things like Draft Amnesty days. Despite all the valid criticism and recent events, EA is pretty great and I expect to continue to have 'EA' on my twitter bio.
18

Thanks for posting this Akash! I had read the initial comment thread and was looking forward to your response