TL;DR
- Respira Health are seeking $84k to pilot and begin scaling a virtual treatment program for Chronic Obstructive Pulmonary Disease*, the second leading cause of death in India and fourth globally (3.5 million annual deaths).
- Our treatment isn’t new, but our delivery model is. Pulmonary Rehabilitation (PR) can cut mortality risk by 9% in just 3 sessions and is a well-evidenced treatment programme for COPD; it combines specialised physiotherapy exercises, education on health habits, and psychological support. PR delivered virtually in high-income countries has been shown to be just as effective as in person, but this is yet to be rolled out in low- and middle-income countries (LMICs) where 90% of deaths occur. We are changing this by delivering PR in India using a WhatsApp chatbot and virtual physiotherapists (think Kaya Guides for respiratory rather than mental health!).
- We’ve already tested our WhatsApp chatbot approach in India. After thorough research and 30 hours of interviews with patients and healthcare professionals in India, we ran our first proof of concept test: we launched a short education program on the main symptom of COPD, breathlessness, using a WhatsApp chatbot. With hospital referrals and Facebook ads, over 140 breathless individuals in our target demographic signed up, demonstrating sufficient demand, feasibility and accessibility for us to begin our pilot.
- We’re in the midst of pilot preparations. We’re now in the process of creating a full 8-week programme of PR content; hiring physiotherapists to support participant screening, monitoring and assessment, building our WhatsApp chatbot, and fundraising for 2026.
- More money you say? Seed-funding in April covered around half of our pilot budget and we’ve subsequently closed most of the remaining gap. Now, with just $23k we can complete a full pilot, lay the foundations for scale and enable further fundraising (runway to June 2026). With $84k, we would be able to more quickly scale-up post-pilot (runway to September 2026).
*Chronic Obstructive Pulmonary Disease (COPD) is a progressive lung condition that can lead to respiratory and heart failure if left untreated. In India, air pollution is the leading cause, while tobacco smoking accounts for only about one in four cases.

Who are we?
Oli Munns and Rowan Lund formed Respira Health in April 2025 through AIM’s Charity Entrepreneurship programme (a platonic dating show for the impact seeking). Prior to this:
- Oli led national digital health projects in the UK Department of Health after an early career at Adobe and has strategy and delivery experience in health nonprofit roles across the UK, Nicaragua, and Nigeria.
- Rowan ran and scaled the operations of Family Empowerment Media, an AIM-incubated digital health NGO, in Nigeria and managed operations and projects for multiple animal welfare and environmental charities.
Why COPD, digital PR and a focus on LMICs?
- COPD carries a significant burden as the fourth biggest killer globally, responsible for 3.5 million deaths per year. It is progressive and debilitating - characterised by breathlessness, coughing, and repeated infections. It often leads to social isolation, economic hardship, and psychological distress.
- Pulmonary Rehabilitation (PR) is a simple and well-evidenced standard treatment. PR consists of specialised physiotherapy exercises, education on health habits, as well as smoking cessation and mental health support. Despite the fact that PR can cut mortality risk by 9% in just 3 sessions, fewer than 3% of people who would benefit from it actually have access; this is primarily due to limited healthcare capacity and insufficient medical training.
- Digital PR is very promising - shown to be just as effective as in person, with 23% higher completion rates, but for a fraction of the cost. We estimate that the average patient who completes this programme will gain over six months of healthy life.
- LMICs account for 90% of COPD deaths. We are focusing our efforts on India where approximately ⅓ of all COPD deaths and disability-adjusted life years (DALYs) occur, where smartphone ownership and digital literacy are relatively high compared to other LMICs, and where the treatment gap remains very high. We aim to develop a replicable model here that can be scaled across other LMICs in the coming years.
- Cost-effectiveness looks very promising given the scalable nature of this intervention and the health effects listed above. Our initial cost-effectiveness analysis (CEA) projected $20 per DALY at scale. This was in April, and since then we have learnt a lot of new information which will likely change our CEA projections. For example, we’re more confident that we can treat people with mild to moderate COPD than before but less confident that we can treat people with severe COPD (we originally only modelled for severe COPD). Also, we think our original estimates for digital literacy levels in India were too far conservative. Our pilot will help us investigate some of our remaining uncertainties so we plan to update and share a revised CEA incorporating all our learnings from Year 1 in spring/summer 2026.
What have we done in our first six months?
We learnt. We spent several months in India, conducting 30 hours of interviews with patients and healthcare professionals to understand their needs, identify existing treatment options, discuss barriers to more effective care being provided, and explore if and how more digital support could be implemented. Our full scoping visit is written up here.
We tested. We developed and launched an educational programme on the topic of ‘breathlessness’ with the support of several local physiotherapists. Recruiting patients from hospital referrals in Mumbai and Delhi, as well as running adverts on Facebook to reach people across the country, enabled us to test the following uncertainties in the early stage of our Theory of Change:
1. Can we reach patients online and via. hospitals?
- Online - Yes. We received over 200 clicks to our chatbot per dollar spent. Although not all of these individuals suffered from breathlessness, we were able to optimise our ad-targeting as we learnt which ads performed better and which audiences best met our key criteria.
- Via hospitals - Yes. Of the 12 hospitals and clinics we met with, we saw referrals from 7 and are in active discussions with some of these about further collaborations for our full digital PR programme. Many already have existing referral routes to in-person PR however, so we’re also exploring partnerships with hospitals lacking referral routes where we hope to see greater benefits.
2. Can we build an appropriate digital intervention without software development backgrounds?
- Yes. It was quick and easy to create the chatbot interface for our educational programme using the no/low code platform Turn.io. We are confident that using this platform for our pilot will allow us to deliver the content effectively, interact with patients, and build an effective data pipeline for Monitoring, Evaluation & Learning, and impact measurement.
3. Will COPD patients over 40 years old have sufficient digital literacy to engage with this?
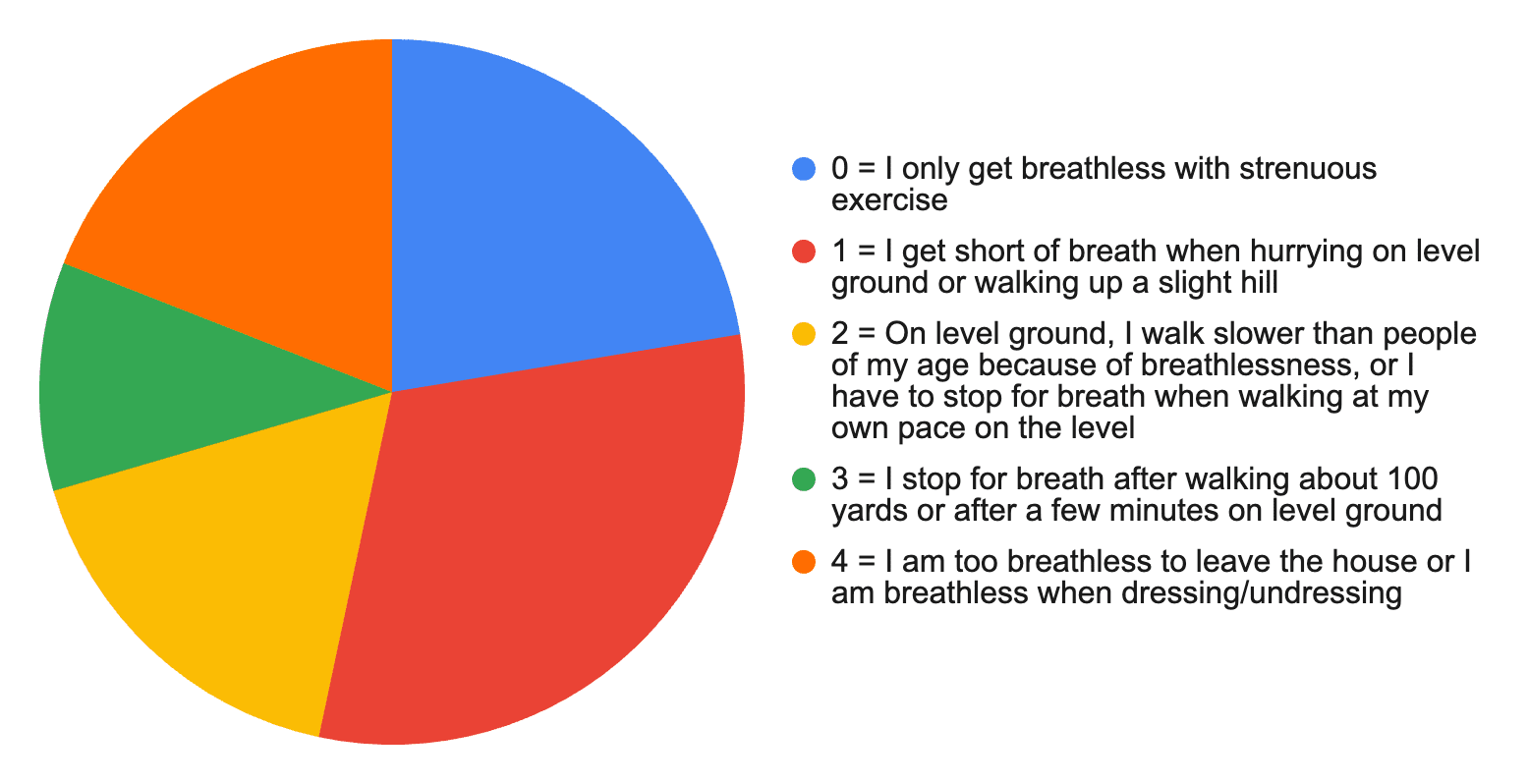
- Yes. When advertising to 40-64 and 65+ year olds, we achieved click through rates (CTRs) of 13.2% and 12.8% respectively. Benchmarks for CTRs are usually 1-2%.
- Yes. On average 18% of those opting in completed our short programme. This was generally higher for those referred from hospitals (~30%) compared to recruited online (~14%).
Reported breathlessness for those opting in to our educational WhatsApp chatbot
(78% of those opting in reported at least some shortness of breath using mMRC scale).

What’s next?
A digital PR pilot! 🎉
We’re ready to build the full programme we plan on scaling to test feasibility and effectiveness. Preparations are well underway. We’re developing an 8-week programme which will use the WhatsApp chatbot to guide patients through exercises, education, and symptom tracking with automatic reminders and motivational messages. Alongside fundraising, we are focused on:
- Hiring. Local physiotherapists will conduct initial screening, ongoing monitoring, and final assessments with patients virtually. Whilst such thorough physiotherapist oversight of each participant is less scalable, we think it’s important to prioritise patient safety, comprehensive data collection and gather qualitative feedback to refine our approach at this early stage.
- Programme content. Using WHO & NHS approved resources adapted for an Indian audience by local medical professionals, we are developing 24 sessions (3 sessions per week for 8 weeks) of exercise and education content delivered via video in English and Hindi, making it more accessible.
- Digital development. In the coming weeks, we will design, build, and test the WhatsApp chatbot which participants will interact with during the programme. The chatbot will not only deliver the content to individuals, but will also enable us to directly capture metrics on user engagement, satisfaction and self-reported health outcomes to inform our programme refinement and iteration.
What do we need?
Room for funding
We raised $110k in seed-funding in April 2025 (about half our year 1 budget). Following our successful scoping visit, we have been able to raise an additional $66k. We are now seeking:
- $23k to complete the pilot.
- Up to $84k for runway to September 2026 so we do not have to continue fundraising during the pilot for our scale-up.
We’re also always looking for useful connections. If you have connections in India, specifically government health officials, hospitals, pulmonologists, respiratory physiotherapists, potential funders, or suggestions for who else you think we should talk to - feel free to reach out to oli@respirahealth.org. You’re the best.
Thanks for stopping by.
Oli & Rowan
Really excited about this—having chatted extensively with Oli and Rowan, they mean business! Also quite excited to see lung health take off more and more as a cause area, could be the new lead, ya never know :)
Thanks for the write-up! Great to learn more about how you're progressing.
Is there a tax-efficient way to donate from the UK?
Thanks Jacco, hope you found it useful and we appreciate your interest in supporting us! In general, no, unless you have a Donor Advised Fund (DAF) or similar as we operate through a US registered 501(c)(3) fiscal sponsor at the moment.
Thanks Oli.
Is there anyone in the US that is willing to do a donation swap with me? I can make a donation to a UK-registered charity (or anything via GWWC) that you were planning to and you can make one to Respira on my behalf :)
It looks like Donation Swap has retired, sadly.
Edit: Jason and I have succesfully arranged a donation swap
How much were you wanting to donate? I am in the US and have some capacity to do swaps in odd-numbered years (although others may have more capacity).
£350+giftaid, so £437.50 total (~$580)