This post highlights how much the European Union could have saved from the Covid-19 pandemic if it was better prepared against airborne diseases. It addresses two complementary methods: biohardening critical infrastructure and personal protective equiment. Together, they would cost roughly 20 billion euros, which is a minor cost in comparison to the estimated 3 trillion euros the EU spent and lost during the crisis. My aim is to show that biosecuirty prevention is not just a way to save lives, but also economically favourable. Thus, making it easier to implement institutionally.
Background
Covid-19 was the trial by fire of contemporary times in terms of coping with pandemic risks. It showed how unprepared the world was to such an outbreak but also was a cautionary tale for more dangerous diseases that could arise in the future. Nonetheless, many cooperative actions and programmes came out of this crisis, vaccines never developed so fast, and campaign methods evolve or were tested to increase efficiency. It was a lesson-learned for the EU, which developed further its supranational governance model to manage the crisis. Still, policymakers lacked a hands-on approach to planning strategies.
A great weakness was calling for funding without provisional assessment of how much was needed to fulfil it in a timely manner.
Nowadays, most water and foodborne diseases are adequately detected and treated, yet humans remain vulnerable to airborne ones, in particular in enclosed spaces where groups of people remain static for extended amounts of time. The aim of biohardening indoor spaces focuses on this vulnerability through the development of biological "firewalls", such as Far-UVC lights. While the installation of lights is contingent with many variables the population has no control upon (lawmaking, funding, etc.), individual action can also enhance preparedness with the use of Personal Protective Equipment (PPE). Thus, an additional recommendation would be the stockpiling of fit tested elastomeric half-mask respirators (EHMR) and training for adequate use.
Costs? What costs?
The benefits of preventive measures have been researched scientifically, but then why are governing bodies not acting on it yet? I think it is because of the costs, and I decided it was time to run the numbers.
Estimations will take Covid as the reference for the sake of simplicity. Compared to the NextGenerationEU, which represented about 637 billion euros,[1] the GDP losses nearing 2 trillion euros,[2] the healthcare sector costs shooting up between 2020 and 2021 to cope with the crisis was of 133 billion euros,[3] which are not even accounting for the human costs, both in terms of DALYs and psychological harm. The total costs are about 2.77 trillion.
Far-UVC
The light, which appears purple to the human eye, could be the future of health and people’s quality of life. They are much less harmful to the skin than UVA and UVB, and powerful germicides. When used appropriately, following the installation guidelines, they successfully “reduced airborne bacteria by 98.4% in a room-sized chamber”.[4]
The acquisition, transport and installation of Far-UVC lights in strategically targeted spaces could drastically reduce contagion. This estimation accounts for necessary venues: grocery stores, transportation hubs (train/metro stations, airports), vehicles (trains, metros), education (schools, universities), workplaces (offices, etc.) and care facilities (hospitals, retirement homes, etc.). It considers they represent the weakest points where people pass through or gather. The focus is solely on the EU, such as accounting for French overseas territories as well.
To be honest, because I have no funding, nor time on my hands to check precisely how many venues have to be equipped, the cost estimate in this section was made using Claude Sonnet 4.6.[5] I made assumptions to simplify the reflection, such as the high demand for devices means that a discount would be applied, and I consider this discount can compensate the installation costs of the lights. The total cost engaged to cover all necessary areas was estimated at 15 billion euros.[6]
Aftereffects of this adoption are, on one side additional energy costs and a need for lamp replacement after a certain time, they are estimated at 1 to 2 billion euros a year. Nevertheless, a positive outcome would be the rarefication of illnesses overall, such as the common cold. For instance, gastroenteritis occurred less during covid because people finally washed their hands! It means the healthcare spendings would be drastically reduced, probably even halved. Moreover, the far-UVC technology might also become cheaper. Together, these facts facilitate the assumption that the aggregated financial relief could compensate the operating costs.
EHMR
Similarly to cars with emergency jackets, PPE are not serving the purpose of preventing the crisis but limiting the deterioration of the situation. The EU recommend households to have 72-hour survival kits, those could be equipped with masks as well as a small stock of filters. They are reusable, thus less harmful for the environment and less costly than surgical masks. Individuals could acquire them in advance of an event and learn to use them safely in case of a pandemic. It would avoid the rush and competition for PPE as happened during Covid.
The cost of an EHMR is relatively low, considering the acquisition of extra filters, they could be estimated at 60 euros per person.[7] It is a one-time cost over the course of a few years, which is very affordable. Costs at the supranational level will come from subsidies for low-resource individuals, municipal emergency stockpiles and adequate use training.
To facilitate the estimations, a fund could be allocated to subsidise about 15% of the population who could not afford such investment, the emergency stocks could also represent 15% of the local population.6 Then, first aid training costs would be an additional 5 euros for the material and instructors’ updating the modules, considering about 20 million people would receive training per year.[8] In total, the EU PPE fund could be around 4.2 billion euros as a one-time cost for the EHMR and 100 million per year for training.[9]
A few important limitations to this implementation are the need for a cultural change when facing PPE. People were uncomfortable facing surgical masks, or even willing to wear them. Respirators could become anxiety-inducing and clash with people’s aesthetic expectations. Normalisation through exposure and social media influencing could support the transition. Then, adequate fit-testing might have to be updated every few years, and these costs are not accounted for in this estimation. Lastly, the respirators also cover the identity of those who wear them, which could be an issue for personal recognition in sensitive venues, such as banks.
Discussion
Now, what would be the reduction of damages brought about by biohardening and PPE? My estimate would be about that the former would better reduce damage compared to the latter, as it is a top-down implementation method. I made my thinking process clear, so that my assumptions have space to be improved upon, I am open for feedback and more precision to refine the final numbers. I start from the total of costs, then based on the estimated percentage of harm reduction I consider the difference with the one-time price for each action.
Research provides a range for far-UVC light efficiency. 90% viral inactivation in 8 minutes to 99.9% inactivation in 25 minutes.[10] On exposure time, if people spend 10 hours at home, 8 at work, 2 in transport, so it leaves 4 hours of exposure elsewhere. I consider that people living alone would be protected 83% of the time, as the high estimate, and 41% if in a shared-living space. I am considering hazards such as power shortages, bad maintenance, etc. to reduce efficacy to 90%.
Estimated for the masks are lower, considering 75-90% population has and can use them, their efficacy is 95 to 100%.[11] However, the issue is to find people willing to wear them, which ranged from 25 to 75 percent of the population during Covid for regular masks, based on socio-cultural norms.[12] Considering personal biases, whether pro- or anti-, it could be considered as transferrable in case of crises: there will still be people concerned for their families or scared of germs, as well as conspiracy enthusiasts or careless.
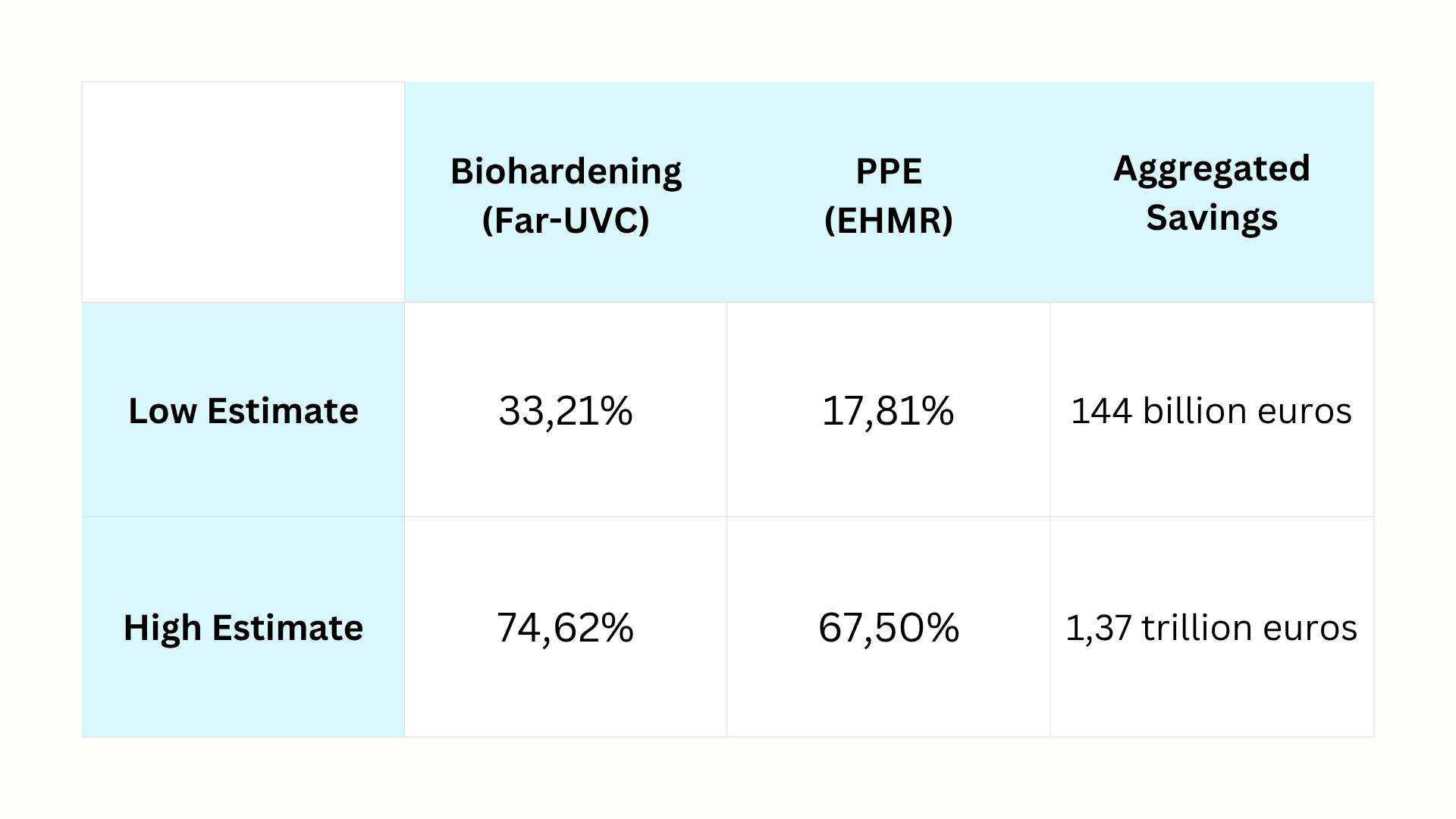
Table: estimates highlighting EU Covid savings if there were biohardening and PPE stockpiling, Savings = Estimate UVC * Estimate PPE * Costs (3 trillion) - Implementation Price (~20 billion)
The wide range of savings (from billions to trillions) come from individual case-by-case disparities, namely who will wear a mask or in which condition do people live, it does not reflect disparities in costs.
Further limitations can be drawn from asymmetric capabilities within the EU, such as the vast gap between Germany or Sweden on the one hand and Malta or French overseas territories on the other. These differences are relevant in terms of resource availability for funding, implementation capability, as well as national culture. Some populations may be less inclined to accept directives based on claims about limitation of liberties, anti-EU sentiment or even conspiracy.
The estimation provided is far from fully “Pandemic-Proofing” the EU, but it proposes a preliminary assessment on how costs could be saved from adequate preparation and adoption of biosecurity safeguards. The complementary impacts of the two solutions highlight how individual agency, as well as policy implementation are indivisible in times of a health crisis and all need to participate to make society safer. Many assumptions have been made and should be corrected by further study, my aim was to provide a prototype to improve upon.[13]
Why would billions be spent on far-UVC and EHMR rather than anything else, such as pandemic surveillance or additional vaccination campaigns? Firstly, the EU already has Eurosurveillance (weekly journal on epidemiology), EpiPulse (online portal on infectious disease data), and is testing Epi+ (multi-hazard monitoring platform). Infections are efficiently documented, which is reassuring. From my perspective, since such reactive surveillance systems already exist, more preventive actions need to be taken to avoid crises from even arising and lighten the burden on these frameworks. Secondly, vaccination programmes can only function if the disease is known and studied. In case of a future pandemic, preventive measures can drastically reduce the contagion rate and leave more time to scientists to research and develop cures or vaccines. Therefore, I am in favour of complementary action, they are not mutually exclusive!
Special thanks to Alex Borwick and Katiana Uyemuraa for their feedback on this piece.
I did 5 in my life, my roommate 1. We are 25, from Western Europe, it is fair to assume it may be less frequent for most people: I assume 1 in 3 person gets first aid training every 8 years.
BLUF:
* To determine whether AI is ‘improving exponentially’, ‘hitting the wall’, or any other claim which involves a quantity or magnitude (e.g. ‘This model was a big leap/small increment’). We need a good y-axis: an interval scale of AI capability which means +1 unit always represents the same degree of ‘how much better’, in the same way +1 degree Celsius is always the same amount of ‘how much hotter’.
* Yet there is no good y-axis for AI capability. All our...
Summary
* The animal welfare movement has already seen an influx in funding and should prepare for the possibility of more.
* The EA Animal Welfare Fund is encouraging those working in animal advocacy to actively set aside time and resources now to concretely plan for scaling sustainably, and we’ll support you in doing that.
* We’re requesting advocates set concrete ambitious goals and submit plans t...
Public service announcement
1. Applications are now open for our first ever round of the Charity Entrepreneurship Incubation Program dedicated exclusively to animal welfare. Learn more about what’s different this round here and apply...