People have been saying all kinds of wild stuff about the new coronavirus. I work in biosecurity and have been following the outbreak since the beginning. What follows is my best attempt to communicate what we know about the virus, and how to prepare, with my family and friends. I thought I would share in case others have been looking for a similar document.
This is *NOT* intended to be a detailed, rigorous justification of the preparation measures I've outlined, nor an authoritative statement on the best current estimates for epidemiological parameters. Instead, I try to be as straightforward as possible, cite only the action-relevant details, and align with the best recommendations I've heard from the EA biosecurity community as well as experts writ large.
Caveats aside, I'd be interested in feedback on this purpose, including whether I am missing sensible prep measures, have the right tone for sharing widely, or am wrong about the facts. I'm happy to provide more technical justification in comments.
Here is the draft. I'll be updating it as we have more info and I have more time to include sources, so go there for the most recent version. The first draft is included below for convenience.
If you'd like, please feel free to copy, modify, etc and share with your own family.
Coronavirus in brief (work in progress)
Bottom Line.
- Coronavirus is significantly worse than the flu, but not the zombie apocalypse. No need to panic, but it probably makes sense to prepare.
- It is going to affect day-to-day-life in western countries, including the U.S.
- You and your family will probably face personal risk of illness by the end of the year.
- You can prepare by
- Stocking ~1 month of nonperishable food and other necessities, and 3 months of medications.
- Relocating away from dense cities and/or shifting to working from home, if possible.
- Learning how to properly wash your hands, and practicing not touching your face.
- Avoiding travel after March of this year, and/or planning with cancellation option.
- Making plans to care for and protect the elderly from exposure to the virus.
- Buying and carrying hand sanitizer, and using it frequently (every 30 min outside your home, before you eat or touch your face).
- Wiping commonly contacted items (phone, keyboard, headphones etc) down with disinfectant regularly.
- Avoiding crowded places (e.g. concerts, subways, theatres, buses, airports etc) without protection.
- For essential travel, buying N95 respirators, if you can, and learning how to use them, including shaving facial hair.
~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~*~
What does the virus do?
- The virus causes coughing, sneezing, fever, pneumonia, and in severe cases kidney failure and death.
- 80% of cases are relatively mild. The rest look like moderate to severe pneumonia.
- Approximately 1% of people who catch the virus die.
- After symptoms show, it takes 3 weeks - 1 month for severe cases to resolve.
- Risk is much higher for people over 40.
- Children appear to be relatively unaffected.
- Men may be twice as susceptible as women, although it is too early to tell with confidence.
- Immunity may not last long, and no-one has it to start with.
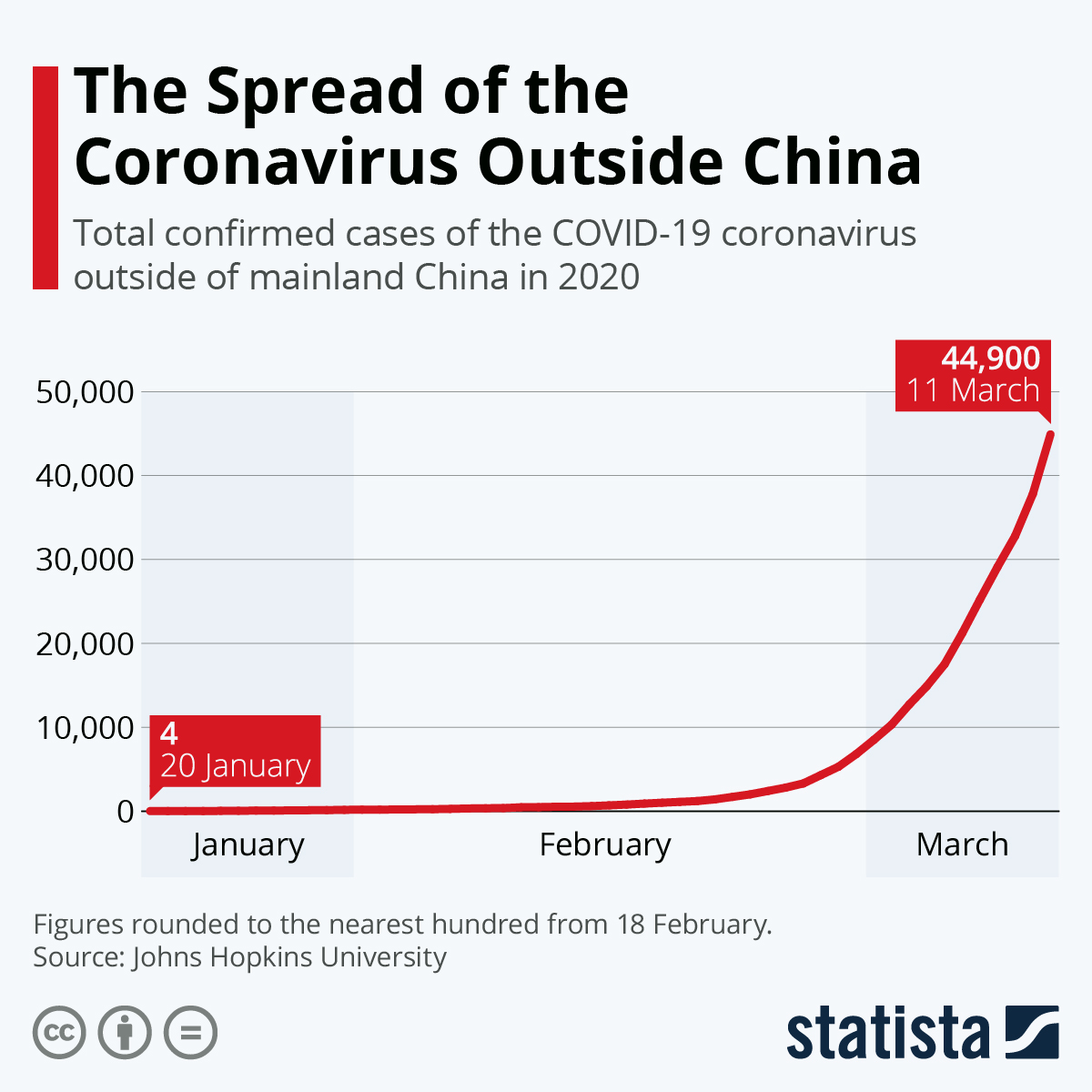
Where is the virus now (Feb 28)?
- 80,000+ cases worldwide, most in China. 2,800+ deaths.
- 23 countries have more than 10 cases outside of China.
- Japan, Iran, Italy, and South Korea all had an exponential growth of cases from 10s to 100s in less than a week.
- 60 cases in the U.S. 1 case, in Northern California, is likely the first spread without link to China, suggesting the virus is spreading undetected in the United States.
What do we know about the virus?
- It likely arose from a crossover, or “zoonosis” from animals in China, sometime in late November early december of 2019.
- It is most closely related to a virus called SARS which caused a small epidemic in 2002. It is also related to viruses that cause the common cold.
How does the virus spread?
- Probably similarly to the flu. Being within 6 feet of a cough or sneeze, touching a surface that has been coughed on and then touching your face, or eating food that has been coughed on are all ways to spread the virus.
- Relatively quickly. Approximately doubling the number of infected people every week.
- The virus can probably survive on many types of surfaces for 2-7 days.
- Some people who are infectious and can spread the virus do not show visible symptoms.
- It takes ~5 days for symptoms to develop.
Can we treat it?
- Not right now. No vaccine or approved medical countermeasure.
- Supportive care like mechanical ventilation can significantly decrease risk of death if ICU rooms are available.
- An antiviral, called remdesivir, is in clinical trials and shows some signs of efficacy.
- Historical timelines for new drug / vaccine rollout suggest mass availability in 2021.
Shouldn’t I be more worried about the flu?
- No. This is worse.
- The flu kills 0.1% of infected people. This kills ~1%. That is 10X worse.
- The coronavirus spreads a little faster than the flu.
- You have some natural immunity to flu even though each season the strain is different. You probably have no immunity against this coronavirus.
- We have a reliable vaccine against seasonal flu. We will not have a vaccine or effective treatment for coronavirus for some time.
- Seasonal flu is very well characterized and understood. This virus is still under intensive study, and all the numbers I give have uncertainty, which means that it may be worse than our best guess. Long-term effects of catching the virus are unknown.
How can I think about my and my family’s risk?
- Look at these charts for risk of death by age group.
- Consider risk factors (source) which make the disease more dangerous, such as cardiovascular disease, diabetes, lung conditions + smoking, high blood pressure, and cancer.
- Think about the population density of places you go to regularly. Ask yourself: “How many people have been here in the last week?”. Avoid places where that number is large, and/or take extra precautions.
- Think about exponential spread. In the early stages, it will be doubling every week approximately. Really think about that- it means the risk is about 2X higher each week this continues. So it’s twice as safe to travel April 1 than April 7. And twice as safe on April 7 as the 14th. I find that extremely counter intuitive, and chances are you will too.
This all sounds crazy.
- Yeah, it does. The info I’ve presented above makes this look like probably the worst pandemic since the 1918 Flu.
- However, what’s presented above is an aggregation of facts and high-quality estimates from the scientific literature and expert recommendations, as best as I could find them.
- The outlook presented here is largely shared by experts at: the CDC, the World Health Organization, the Harvard School of Public Health, the Johns Hopkins Center for Health Security, a biosecurity summit I recently attended, and by most of my colleagues in the biosecurity space.
- Unfortunately, I think this is the world we live in.
Other resources


{kind=link}
{kind=link}
{kind=link}
A friend pointed me to a study showing a high rate of chronic fatigue in SARS survivors (40%). I did a quick analysis of risk of chronic fatigue from getting COVID-19 (my best guess for young healthy people is ~2 weeks lost in expectation, but could be less than a day or more like 100 days on what seem like reasonable assumptions. ) https://docs.google.com/spreadsheets/d/1z2HTn72fM6saFH42VKs6lEdvooLJ6qaXwCrQ5YZ33Fk/edit?usp=sharing
Thank you for doing this. Has been on my list to look at for a while and am really glad we have numbers to work with.
Big source of uncertainty is how long the fatigue persists - it wasn't entirely clear from the SARS paper whether that was the fraction of people who still had fatigue at 4 years, or people who'd had it at some point. Numbers are very different if it's a few months of fatigue vs rest of your life. Not sure I've split up the persistent CF vs temporary post-viral fatigue properly