Comments
Family Planning mHealth Intervention - Initial Research by Lafiya Nigeria

7 min read
Each year more than 220 million women worldwide have an unmet need for contraception, resulting in over 300,000 maternal deaths from pregnancy-related complications. Unmet need for family planning can be attributed to insufficient knowledge about family planning and access to family planning services.
During our pilot program in 2022, we noticed that this problem is only more prevalent among rural women. Rural women in Nigeria have fewer years of education, lower income, and worse health outcomes than their urban counterparts. The prevailing barriers to access family planning information and services faced particularly by rural women are: lack of trained medical personnel, stockouted healthcare facilities located far from their communities. For example, Kebbi state has only 144 doctors to support the population of over 5 million people, which translates to 1 doctor per every 50,000; a far cry from the WHO recommended figure of 1 doctor per every 1000 people.
Lafiya Nigeria offers in-person family planning counselling and administration of contraceptives free of charge. This model has proven to be highly cost-effective and is currently replicated in another state. However, we have identified one missing part of the solution - an mHealth component that can be used to offer educational information about sexual and reproductive health, send reminders for next doses of contraception, connect patients with the locations of family planning service providers, and provide up-to-date information about the stock levels. We believe that an mHealth component has a potential to become a key part of our comprehensive solution for a cost-effective family planning solution.
The proliferation of mobile phone ownership in LMICs has enabled digital technologies to provide family health information among users living in hard-to-reach areas. Mobile health solutions have been found to reduce costs of health care whilst improving the quality of care. The evidence has been so robust that it has resulted in the WHO releasing the guideline Recommendations on Digital Interventions for Health System Strengthening and endorsing the use of mobile health technologies in interventions targeting communities in LMICs.
The previous uses of mHealth family planning platforms showed their effectiveness in the increase of the contraceptive uptake. The users of mHealth platforms could seek information about family planning and related resources from the comfort of their home rather than going to a clinic or a health care provider.
Family planning mHealth interventions have shown promising results across different demographic and geographies, adopting unique solutions to best match the needs of the targeted communities:
There is a strong evidence base that mHealth interventions can result in the significant increase in contraceptive uptake. The level of impact achieved depends on the exact program design and the needs of the targeted demographic.
Lafiya Nigeria team has identified the existing gaps in the current family planning landscape and the potential of a well-designed mHealth component to address the barriers faced by women with unmet need for contraception. An example of a mHealth solution within the existing Lafiya Nigeria model could fulfil some or all of the following functions:
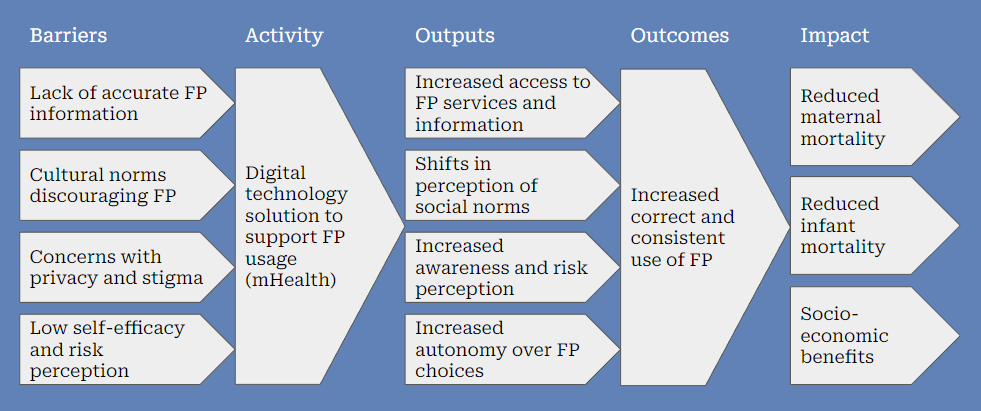
The following theory of change shows the impact of an mHealth component of the Lafiya Nigeria model.
The initial research on this idea has demonstrated a strong evidence base and a good organisational fit to solve the problem. This fit comes from a successful pilot project that Lafiya Nigeria rolled out, culminating in:
(i) a database of rural Nigerian women with the unmet demand for contraception;
(ii) a network of health providers across different clinics and health facilities in over 60% of LGAs within targeted states;
(iii) strong relationships with the Ministry of Health on state and federal level;
(iv) an experienced and dedicated team with a proven track record of delivering global health interventions.
The Lafiya Nigeria team has conducted an initial round of expert interviews from IDInsights and Center for Global Development; and practitioners of mobile-based interventions from India (Suvita) and Kenya (M-Schule).
Those interviews have given us a good starting point to evaluate existing tools and identify any technological challenges this project would entail. We have also recruited volunteers with backgrounds in programming and software development from Stanford and Berkeley to bridge the capability gap within our team.
Our team will now conduct deeper analysis of the identified solutions, including assessing their feasibility, building a cost-effectiveness model, and conducting initial conversations with the state governments to understand how this project would align with their current priorities.
To identify the features and format of the tool, we are seeking to answer the following questions:
We anticipate adding more follow-up and detailed questions as we conduct our in-depth research.
If you are interested in this cause area and would like to support this project, you can help in three ways:

