Supplements with a U-shaped benefit/harm curve like that and different effects in different subgroups aren't appropriate for universal supplementation. This is not that different to trying to add antihypertensives to the water supply.
Like most antihypertensive treatment, potassium supplementation needs to be implemented case-by-case and on a voluntary basis so that the subpopulation that needs less potassium aren't involuntarily harmed.
Supplements with a U-shaped benefit/harm curve like that and different effects in different subgroups aren't appropriate for universal supplementation.
Is this a like a medical rule of thumb?
I'd just imagine that all the other commonly fortified minerals and vitamins are u-shaped in outcomes. Calcium, iodine causing hyperthyroidism. It'd just depend on the risks.
I did already glance at how likely potassium would harm others and you might find the current information interesting:
The studies suggest that so far it seems quite safe. However there could be a mild (1-2) point increase in blood pressure at the low doses for people who aren't hypertensive, which shouldn't impose much risk.
I think that U-curve is narrower with potassium than with iodine, calcium, or fluoride. The consequence of severe hyperkalemia is cardiac arrest so it's quite serious. Most people would have to consume a lot of potassium to get to that point but certain subgroups - people with kidney failure for example - would be susceptible.
And many patients don't listen or they make mistakes. In an opt-in system that is considered their responsibility, but in an opt-out system like you're proposing, bad outcome will be blamed on the potassium fortification program. Not politically viable
Thanks so much for this - I love quick cost-effectiveness attempts and this is an interesting idea - strong Upvote! I agree with @Henry Howard🔸 that the risks and downsides of universal supplementation with potassium are very different from folate due particularly to the potential to worsen hyperkalemiea (even by a touch) in certain groups of people.
Fortification is always a tough sell as is, and in this case with almost certain (if small) downsides in this case it might be almost impossible to implement even with net benefit.
Thx for sharing! Interesting calculation. I did one by myself (with perplexity) and landed at costs of roundabout 500000 Euros per avoided death (50 DALYs). But i can‘t remember all my assumptions which i put in there. One Killer/argument might be: potassium salt and and anti-blood-pressure medication might be some kind of substitutes. So that more potassium salt might sometimes simply lead to less medication instesd of lowering the risk?
My inspiration for doing my back-on-the-envelope-calculation where: https://www.newscientist.com/article/mg26234940-100-how-to-easily-satisfy-your-salt-cravings-without-damaging-your-health/
The article is behind a paywall, but i will send you a working link.
Thx for this calculation!
Just to check—is the 230mg target additive to sodium, or substitutive? I can imagine the interventions would look different if we merely had to fortify food vs start replacing sodium.
In general, I’m hugely in favour of EA considering this (and similar interventions like mandating/favouring sugar substitution). Health issues that face rich countries today are likely already facing poor countries in large quantities and will only get relatively worse as we solve other problems.
It'd depend on the food in question. The analysis however was under the assumption of it being additive, i.e. typical fortification.
I'm not a baker or a cow farmer so I don't know in what situations salt can be replaced with potassium chloride. I think in a lot of cases potassium chloride should be able to be added with limited issues as saltier things tend to taste better.
Napkin Math Analysis - Potassium fortification to reduce Blood Pressure
Ever been to the doctor and have them give you those 2 funky numbers?
That's called blood pressure honey.
Me and @Hussein Khambhalia spent around 2 hours on the weekend to see if we had the ability to calculate the cost effectiveness of something. That weekend we looked into potassium chloride fortification in the US.
Nearly half of adults have high blood pressure (48.1%, 119.9 million). This is defined as a systolic blood pressure greater than 130 mmHg or a diastolic blood pressure greater than 80 mmHg or are taking medication for high blood pressure.[1]
About 1 in 4 adults with high blood pressure has their blood pressure under control (22.5%, 27.0 million).[1]
High blood pressure costs the United States about $131 billion each year, averaged over 12 years from 2003 to 2014.[1]
In 2022, high blood pressure was a primary or contributing cause of 685,875 deaths in the United States.[1]
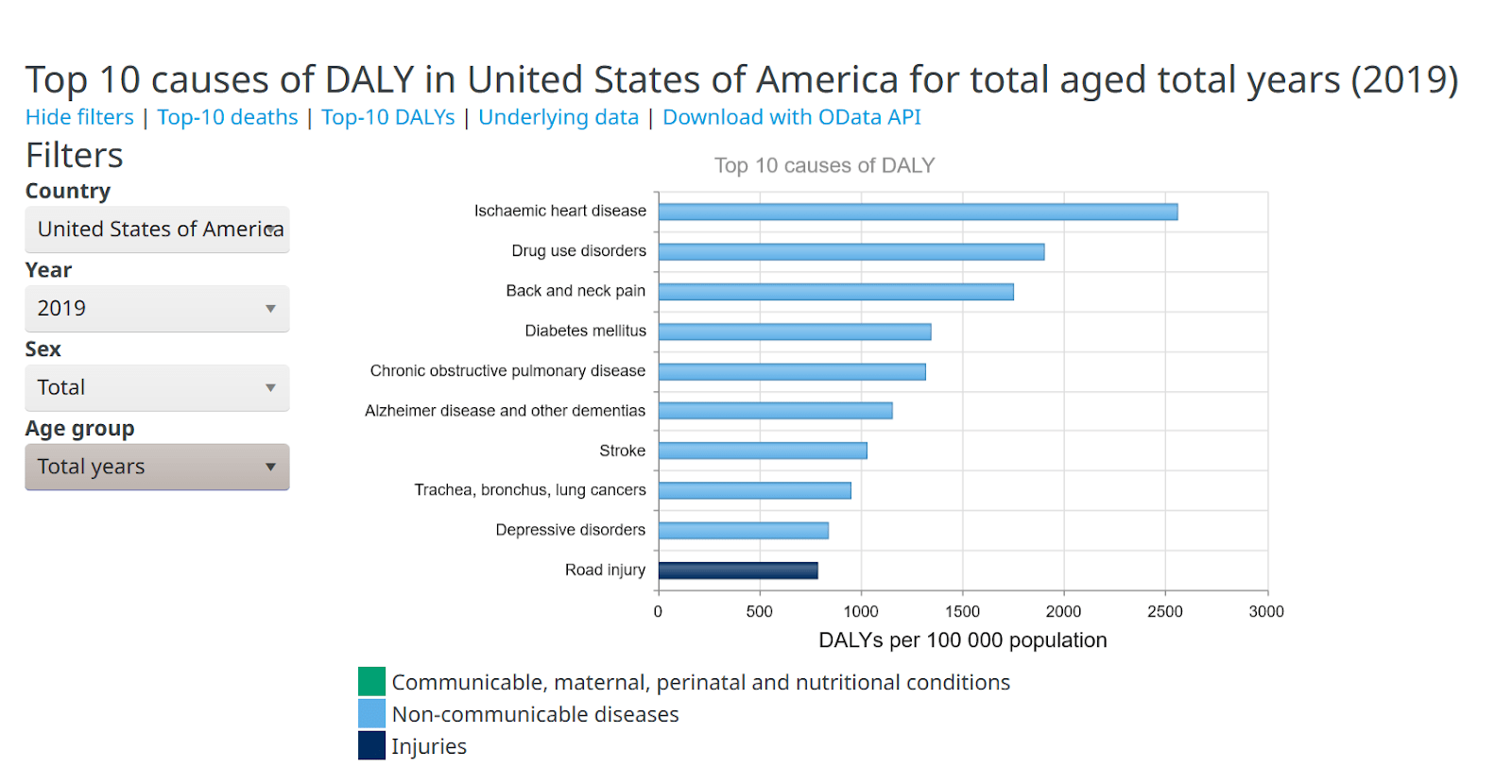
The ones we will look at today are Ischaemic heart disease aka Coronary Heart Disease. And Stroke https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/global-health-estimates-leading-causes-of-dalys
Pulling it out from the data above:
Ischaemic heart disease (Coronary Heart Disease) - 2556.34 DALY rate per 100,000 population
Stroke: 1024.89 DALY rate per 100,000 population
Intervention
Potassium chloride can be used as a salt substitute for food, but due to its weak, bitter, unsalty flavor[2], it is often mixed with ordinary table salt (sodium chloride) to improve the taste, to form low sodium salt. [3]
Every 10 mm Hg reduction in systolic blood pressure significantly reduced the risk ... coronary heart disease (0·83, 0·78-0·88), stroke (0·73, 0·68-0·77) ...[4]
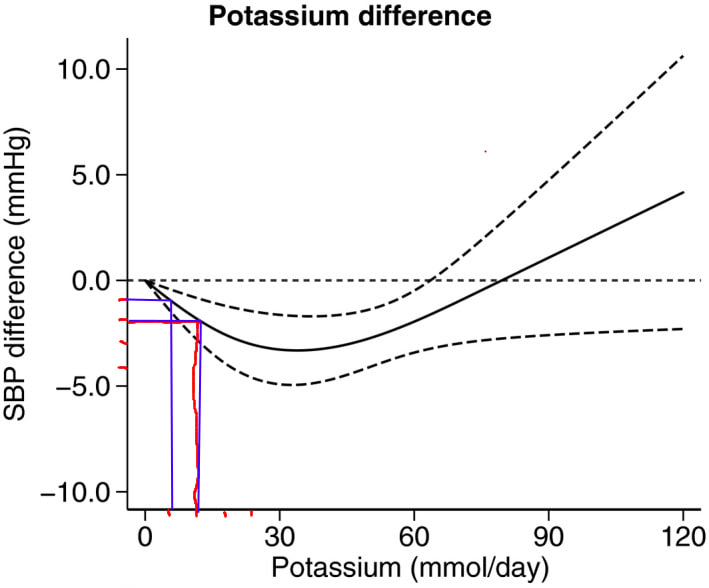
Let's say we attempt to fortify the USA with potassium chloride. 6mmol/day≈230mg potassium≈500mg potassium chloride.
This corresponds to about a drop in Systolic Blood Pressure (SBP) of 1mmHg, which will reduce stroke and CAD risk.
Given that a slice of white bread has around 150mg sodium, it's not unreasonable that we could fortify people's food to hit 230mg a day.
Recall:
Ischaemic heart disease (Coronary Heart Disease) - 2556.34 DALY rate per 100,000 population
Stroke: 1024.89 DALY rate per 100,000 population
The US population in 2019 was 328.3 million.
Therefore, the total burden of CAD and Stroke in the US is around: CAD:2556.34100,000×328,300,000=8,392,464DALYs Stroke:1024.89100,000×328,300,000=3,364,713DALYs
Assuming a linear relationship of the disease risk factors. A drop of 1mmHg in SBP works to reduce the risk of the disease by: CAD Risk:1.7% Stroke Risk:2.7%
Here is an estimate that suggests the cost of fortifying folic acid is linear ~ $1.5 million being the fixed cost. Cheaper than I expected. Thus we are assuming fixed costs are relatively trivial.
Estimates of annual fortification costs for the 140-mcg fortification strategy ($3.3 million) were based on those used by Grosse and colleagues, and those for the two hypothetical scenarios ($6.0 and $10.6 million for 350-mcg and 700-mcg fortification strategies, respectively)[5]
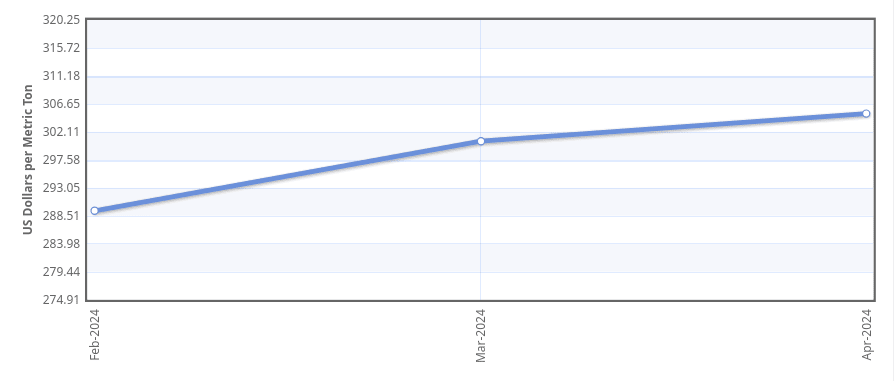
Below we can see the cost of potassium chloride is about $300 a metric ton.
If we try to get 0.5g of potassium chloride to every American that would be about 164,150 metric tons. A naive calculation would give us $50 million as the material cost.
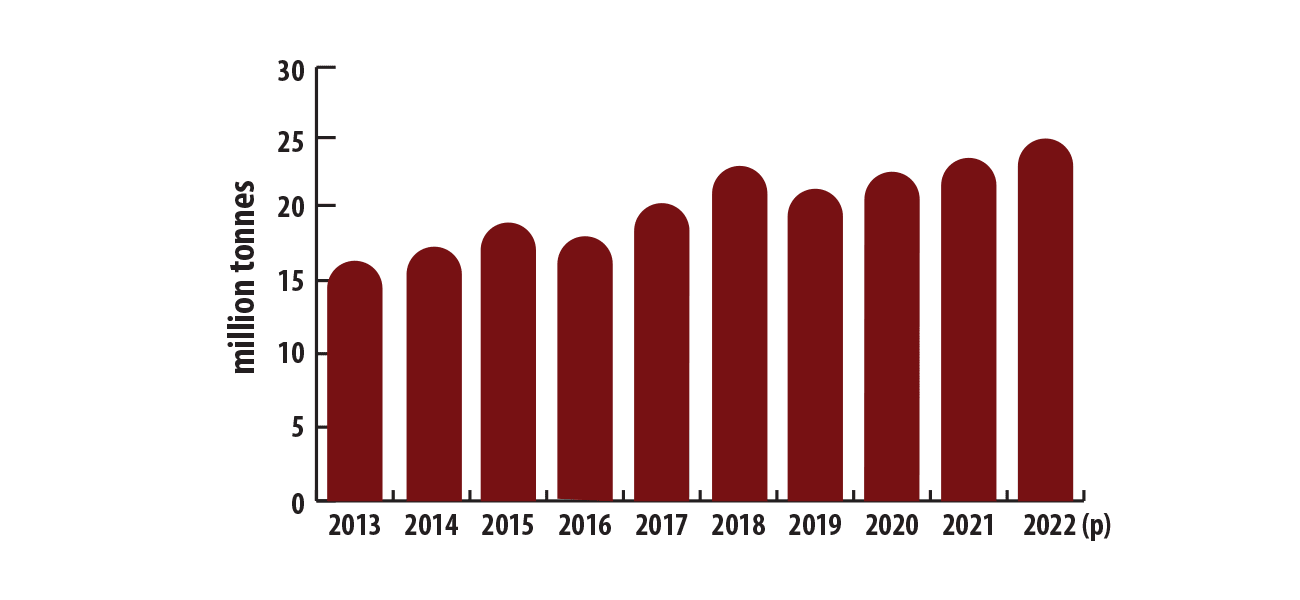
Canada produces at least 25 million tons a year (no idea how much of that is food grade). Which means that we aren't hitting a physical limit at least.
Because I have no idea on the price elasticity of potassium chloride, we will go from the $300 to up to 8x the cost for visualisation purpose.
And the final results:
Program Cost
Cost/DALY
Cost/Life (80 years)
$50 million
$214
$17,129
$100 million
$428
$34,258
$200 million
$856
$68,516
$400 million
$1,712
$137,033
Given that most Western countries value a DALY in excess of $50,000,[6] this seems like an interesting route to look more into?
Problems
I suspect there's a lot of problems, would love to hear your thoughts! Here is a non exhaustive list that I could think of:
Palatability issues
Potassium Chloride food grade manufacturing cost
Potassium Chloride commodity price elasticity
Adverse effects from those who are sensitive to potassium, i.e. hyperkalemia
People who already have low blood pressure
But on the flipside there are things that could make potassium chloride fortification stronger:
Marginal benefit of one less CAD/Stroke victim, i.e. their productivity or getting to spend the resources on their medical care elsewhere. $131 billion a year is a lot.
Reduction in risks for not just Stroke, and CAD but all Cardiovascular diseases
The intervention in another country being cheaper than the US
Conclusion
It was quite satisfying to synthesise a concrete number. LARPing as a bad GiveWell employee was overall pretty fun! I think we might continue + with any feedback.
I hope this inspires others to give it ago, maybe an attempt to recalculate our number more comprehensively or test out another intervention.
As an aside, I hope everyone checks their blood pressure and try to keep it at a healthy number, it's called the silent killer for a reason. Maybe you might try some potassium chloride ;)
BLUF:
* To determine whether AI is ‘improving exponentially’, ‘hitting the wall’, or any other claim which involves a quantity or magnitude (e.g. ‘This model was a big leap/small increment’). We need a good y-axis: an interval scale of AI capability which means +1 unit always represents the same degree of ‘how much better’, in the same way +1 degree Celsius is always the same amount of ‘how much hotter’.
* Yet there is no good y-axis for AI capability. All our...
Summary
* The animal welfare movement has already seen an influx in funding and should prepare for the possibility of more.
* The EA Animal Welfare Fund is encouraging those working in animal advocacy to actively set aside time and resources now to concretely plan for scaling sustainably, and we’ll support you in doing that.
* We’re requesting advocates set concrete ambitious goals and submit plans t...
Public service announcement
1. Applications are now open for our first ever round of the Charity Entrepreneurship Incubation Program dedicated exclusively to animal welfare. Learn more about what’s different this round here and apply...




Supplements with a U-shaped benefit/harm curve like that and different effects in different subgroups aren't appropriate for universal supplementation. This is not that different to trying to add antihypertensives to the water supply.
Like most antihypertensive treatment, potassium supplementation needs to be implemented case-by-case and on a voluntary basis so that the subpopulation that needs less potassium aren't involuntarily harmed.
btw I'm a fan, your vid helped get me sign the pledge last year!
Is this a like a medical rule of thumb?
I'd just imagine that all the other commonly fortified minerals and vitamins are u-shaped in outcomes. Calcium, iodine causing hyperthyroidism. It'd just depend on the risks.
I did already glance at how likely potassium would harm others and you might find the current information interesting:
https://examine.com/supplements/potassium/#what-are-potassiums-main-drawbacks
The studies suggest that so far it seems quite safe. However there could be a mild (1-2) point increase in blood pressure at the low doses for people who aren't hypertensive, which shouldn't impose much risk.
I think that U-curve is narrower with potassium than with iodine, calcium, or fluoride. The consequence of severe hyperkalemia is cardiac arrest so it's quite serious. Most people would have to consume a lot of potassium to get to that point but certain subgroups - people with kidney failure for example - would be susceptible.
Definitely an assumption of mine: but those with kidney issues would already have to be educated on what foods/minerals to avoid I had imagined.
Would you happen to know any other subgroups?
And many patients don't listen or they make mistakes. In an opt-in system that is considered their responsibility, but in an opt-out system like you're proposing, bad outcome will be blamed on the potassium fortification program. Not politically viable
I see, appreciate the responses