Comments
Why is the rate in ocean Oceania so low? I would naively have expected it to be decent but not as good as in richer parts of the world? Is "no data" being coded as "zero occurrence"?

Why is the rate in ocean Oceania so low? I would naively have expected it to be decent but not as good as in richer parts of the world? Is "no data" being coded as "zero occurrence"?
That's not a per capita rate, it's a total count. The population of Oceania excluding Australia and New Zealand is really small.
Thanks! I missed that it was absolute. A rate would make more sense, though I guess absolute numbers do tell us the size of the opportunity.
I am not clear from your explanation on whether health impacts are talking about the effect on the mother or the effect on the stillborn child. If you are considering the effect on the stillborn child, it seems that you should consider increasing reproduction as approximately as good as decreasing stillbirths.
it seems crazy to imagine a baby dying during labour as anything other than a rich, full potential liife lost, but if we extend that logic too far backwards then we might imagine any moment that we are not reproducing to be costing one “life’s worth” of DALYs. Time discounting is a difficult science
It seems to me that you have to accept one of these or the other. Treating a failed conception as ~0 DALYs but a stillbirth as ~5 DALYs doesn't make any sense to me. Either they should both be ~0, or they should both be ~70. But if the 5 DALYs number is the effect on the mother, then that's fair. (Although I'm guessing the effect on the mother would be much smaller than that?)
(I have no comment on the rest of the investigation as it's somewhat technical and outside of my expertise. It looks like you're looking at the right questions, at least.)
Hi Michael. Thanks for your thoughtful comment.
You've highlighted an issue I agree with- that this is something of a grey area where one's personal position on complex moral issues can make a big difference to how effective you think this problem area might be.
I am not clear from your explanation on whether health impacts are talking about the effect on the mother or the effect on the stillborn child.
In the article, I'm defining the health impacts of a stillbirth as the years of health, or healthy life, lost to the child who is stillborn- this, as you point out, is very hard to define. Any health impacts on the mother (not related to economic or wellbeing impacts) were not described particularly fully in the readings I found, although there may be more research that I haven't seen; I suspect they would be hard to entangle from the health problems which may have contributed to, rather than caused, a stillbirth.
It seems to me that you have to accept one of these or the other.
If I was smarter, I'd have a better impression on where I fell on this issue. What I hope to point out in the article is that taking either position to an extreme results in a position that clashes with my, and I suspect many people's, moral intuition. Probably further thought on this is required by people who have more experience with time discounting/health economics/actuarial sciences than me.
If you are considering the effect on the stillborn child, it seems that you should consider increasing reproduction as approximately as good as decreasing stillbirths.
Presumably, some people do think this. I think for me to have a strong position on it I'd have to have strong positions on other, more fundamental moral questions that I haven't come to good answers for.
You're right; surely abortion, miscarriage, and stillbirth are all equally bad for the embryo/fetus/child and should either be counted as 0 or -70 depending on whether you count these as people or not. (Unless there's some kind of Shapley value argument where an abortion of a 5-week embryo counts as only a fractional loss of life because it might have miscarried anyway even if there had not been an abortion, but I don't think anyone is proposing such an accounting here.)
It's frustrating that people downvoted you to -6 agreement but no one bothered to explain what they disagreed with.
Is it your first article like that? And did you write it solo? I'm not into global health, but overall it looks super impressive.
Hi, Liv- yes, it's pretty much my first time doing something like this. I do have some medical background but I haven't got any experience in policy/evaluation/whatever this is.
Fortunately, I had some great help and direction from the Cause Innovation Bootcamp organisers (especially my mentor Leonie), who put together some great materials on how to approach writing like this. It's not where I'd like it to be in terms of completeness but I think we all reached a point where the return on further time invested didn't make much sense.
Thankyou so much for your kind words- it's surprisingly nerve-wracking posting something on the Forum like this, especially for a first-timer.
Hi - thanks for writing this - agree this is a somewhat neglected topic in general. You might want to look at a couple of my papers: a conceptual one (with my father and some perinatologists), and a follow-up empirical one that does actually ask people to try to put numbers on some of these important tradeoffs.
Lastly and probably most significantly, there is obviously the loss of an additional individual who would likely have been economically productive over the course of their lifetime
From a common-sensical point of view, it’s difficult to know exactly where to “draw the line”; it seems crazy to imagine a baby dying during labour as anything other than a rich, full potential liife lost, but if we extend that logic too far backwards then we might imagine any moment that we are not reproducing to be costing one “life’s worth” of DALYs.
There seems to be an obvious route of inquiry to address this quandary, which is to ask what impact a stillbirth has on the number of children a woman has during her life. I imagine some nontrivial fraction of women who have stillbirths go on to become pregnant again in relatively short order, and end up having just as many children as they would have had the pregnancy succeeded. If, hypothetically, 90% of women who have stillbirths go on to have just as many children as they would have without the stillbirth, and 10% have one fewer children, then it seems straightforward to me that we should count a stillbirth as costing 0.1 lives. I don't know actual numbers about how stillbirths impact women's later reproductive choices, but presumably somebody has studied this.
Thank you for writing this exploration of such an important topic. EAs are too often unwilling to follow through on the moral implications of “the sanctity and preciousness of human life” even in the womb.
This topic has the potential to be deeply upsetting to those reading it, particularly to those who have personal experience of the topic in question. If you feel that I’ve missed or misunderstood something, or could have phrased things more sensitively, please reach out to me.
Throughout the review, words like “woman” or “mother” are used in places where some people might prefer “birthing person” or similar. This choice reflects the language used in the available literature and does not constitute a position on what the most appropriate terminology is.
This report is a shallow dive into stillbirths, a sub-area within maternal and neonatal health, and was produced as part of the Cause Innovation Bootcamp. The report, which reflects approximately 40-50 hours of research, offers a brief dive into whether a particular problem area is a promising area for either funders or founders to be working in. Being a shallow report, it should be used to decide whether or not more research and work into a particular problem area should be prioritised.
Key uncertainties
Stillbirths are generally defined as the death of a baby after 28 weeks of gestation but before birth1 (although this definition is not quite universal). Miscarriages, by contrast, are those foetal deaths which occur before 28 weeks of gestation, and neonatal death usually refers to deaths within the first 28 days of life. Stillbirths can occur at any time between 28 weeks gestation and the moment of delivery, but around half of all stillbirths worldwide occur during labour1, the period immediately leading up to the moment of birth.
Stillbirths are likely to have been occurring for as long as there have been births, and occur in other mammalian species at similar or greater rates. However, they have been rising up the global health agenda in the previous two decades, driven particularly by two detailed Lancet review series in 2011 and 2016, from which this shallow review draws extensively.
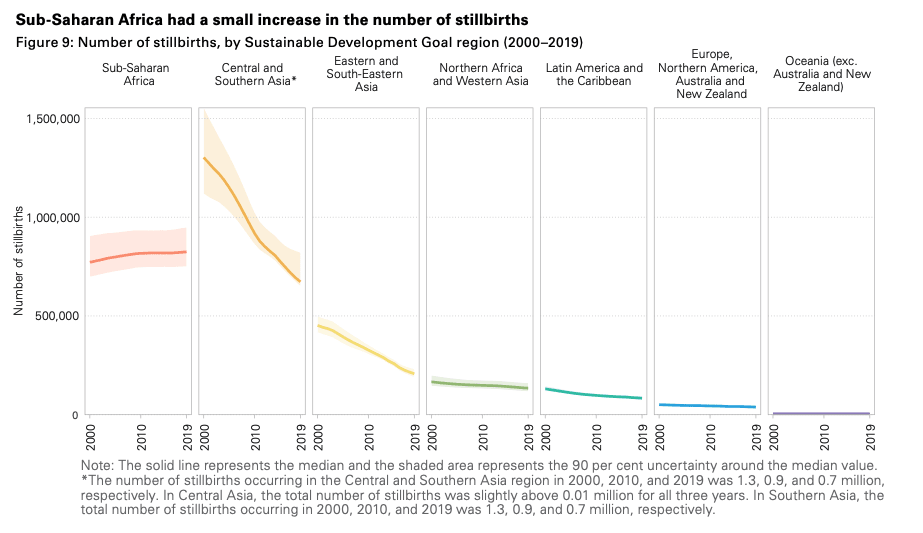
Stillbirths have been declining gradually over time in most regions, with the most dramatic decline occurring in Central and Southern Asia. The number of stillbirths in Sub-Saharan Africa slightly increased from 2000-2019, and by 2030 it is estimated that the majority of global stillbirths will be in this region; at the current rate of progress, it will be 160 years before a pregnant woman in Africa has the same risk of stillbirth as a pregnant women in a high-income country.2
Although any decline in stillbirths is positive, it is notable that progress has been significantly slower than the rate of decline of neonatal and infant mortality.3 It’s not immediately clear why this is, as many interventions which reduce the risk of stillbirth also reduce neonatal and infant mortality, as outlined below.
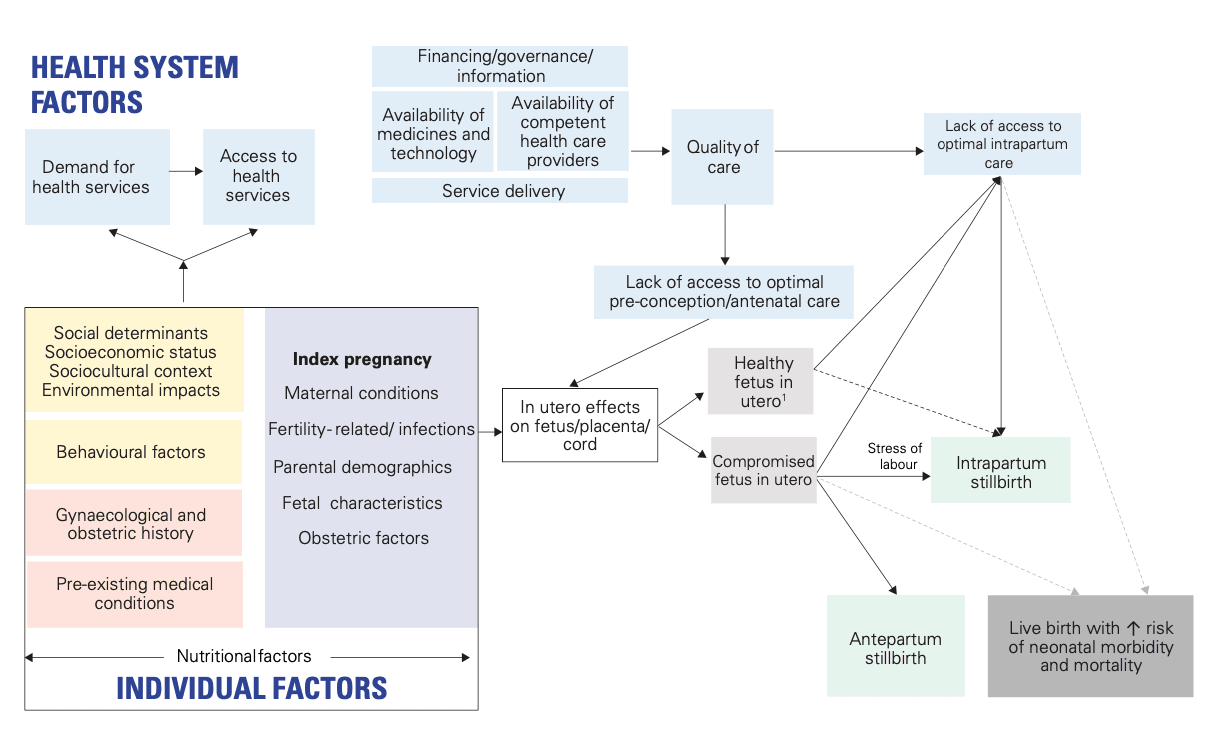
Although it is sometimes possible to pinpoint the precise cause of a particular stillbirth, in most cases the causes are likely to be complex, multi-faceted, and emergent4:
This graphic demonstrates how the health and wellbeing of the mother prior to conception and the strength of the local healthcare system can interact with antenatal health problems to increase the risk of stillbirth; it may be the case that some stillbirths are effectively “caused” many decades before they actually occur. However, a plurality of stillbirths still occur during labour, especially those in the developing world.1
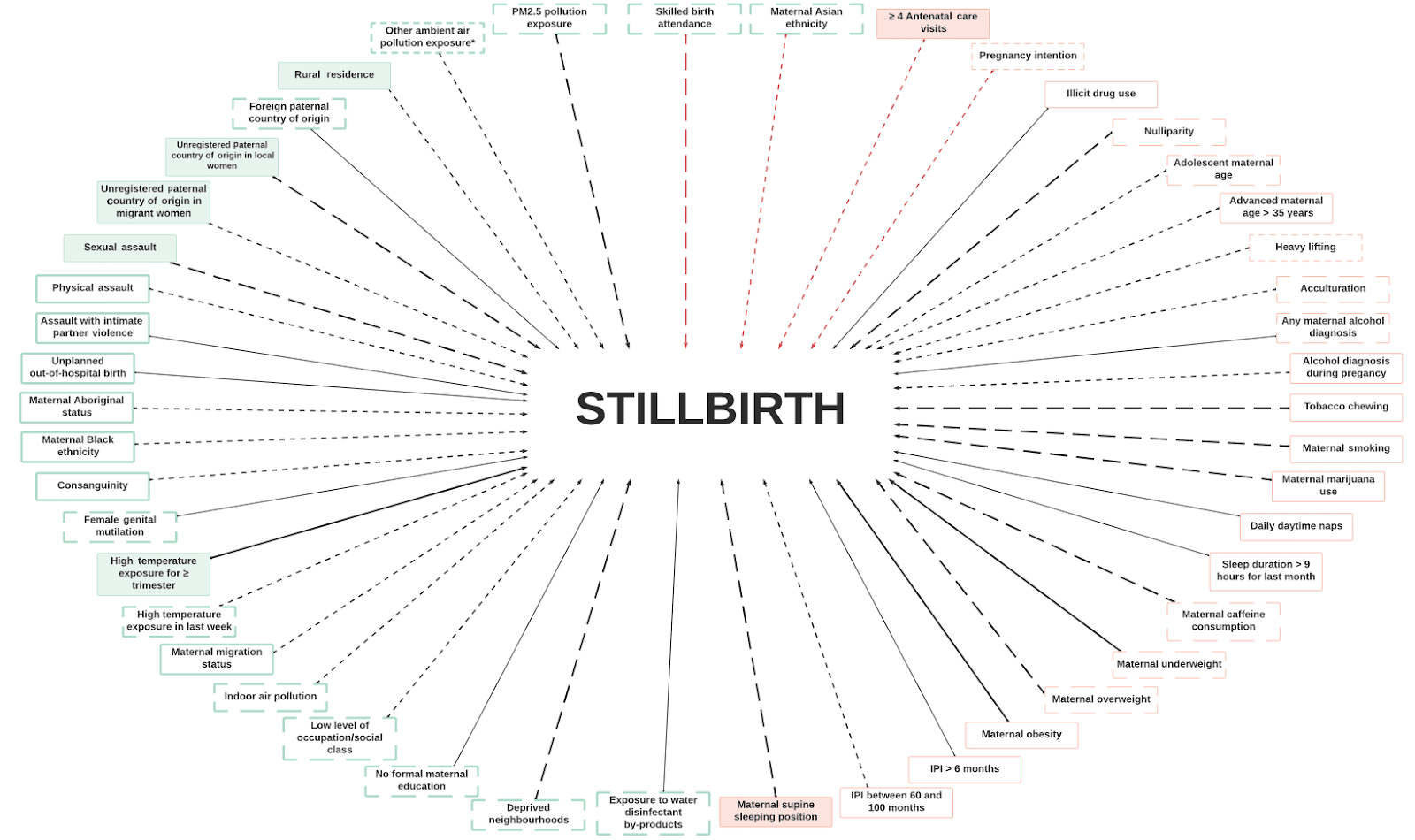
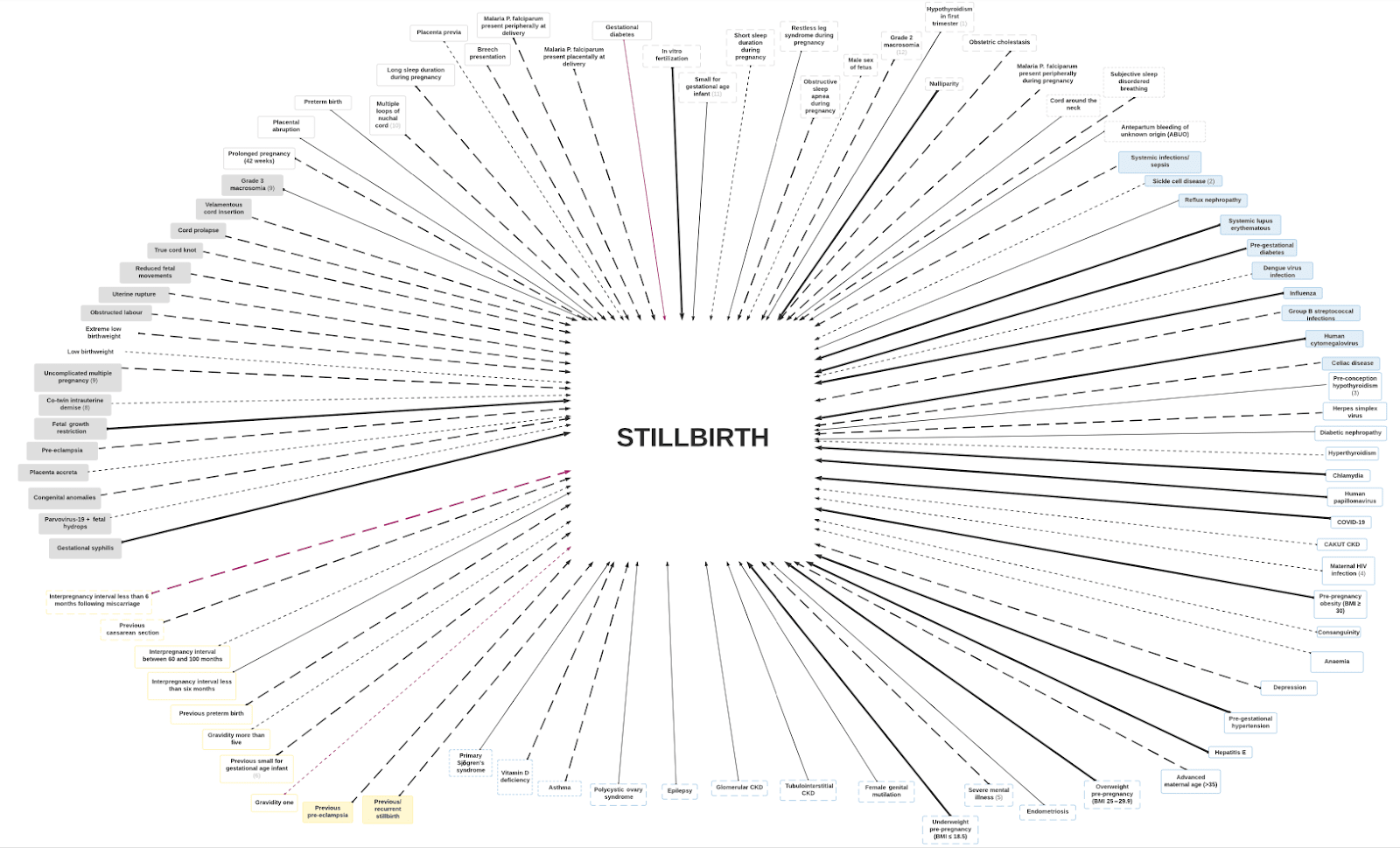
Factors like smoking, excessive alcohol intake, and some pre-existing medical conditions are all known to increase the risk of stillbirth, but attempts to create a gears-level understanding of why stillbirth occurs and how we might prevent it is difficult, to say the least:
Tl;dr- it’s complicated.
There are approximately 2 million stillbirths every year worldwide.2 Even in higher-income countries, the number of stillbirths is usually greater than the number of infant deaths in the equivalent time period5.
Each of these stillbirths has economic, health, and wellbeing impacts which “ripple outwards”, like5 a stone dropped into a pond, from the stillborn child out to their immediate family, the local community, and wider society.
There are direct and indirect income burdens resulting from stillbirth.
Direct income burdens include the cost of post-stillbirth care, which can be borne by governments, insurance companies, communities, and/or parents, and can be anywhere from hundreds to tens of thousands of dollars more than what would typically be paid for a live birth.6 Future pregnancies then tend to cost more as a result of increased monitoring requirements. These costs are likely to vary significantly between contexts, as will the ability of parents to pay them.
Indirect income burdens related to stillbirths include reduced parental earnings, reduced productivity and economic engagement, and potentially increased costs from psychological therapies and further antenatal counselling.6 Many parents reported never reaching pre-stillbirth productivity levels, meaning that the cumulative economic impact of the emotional stress could be significant.
Lastly and probably most significantly, there is obviously the loss of an additional individual who would likely have been economically productive over the course of their lifetime- this is difficult to quantify but could be by some margin the most important consideration, depending on the estimated size of their contribution.
These may be the most difficult to assess because different authors calculate the loss of DALYs from each stillbirth very differently6. Estimates range from 0-86 DALYs lost, with time discounting to around 5 DALYs seeming to be a reasonably common middle ground; this is obviously a very significant range, and as such variation in the evaluators position on this is likely to be the most important factor in their overall evaluation of the impact of stillbirth.
From a common-sensical point of view, it’s difficult to know exactly where to “draw the line”; it seems crazy to imagine a baby dying during labour as anything other than a rich, full potential liife lost, but if we extend that logic too far backwards then we might imagine any moment that we are not reproducing to be costing one “life’s worth” of DALYs. Time discounting is a difficult science and seems likely to vary depending on the context in which the stillbirth takes places as well as on the personal moral preferences and positions of the evaluator. A more defined answer to this question, perhaps similar to GiveWell’s work on moral weights, could be very useful for future evaluation.
There are evident non-economic costs to stillbirths, although these can be difficult to quantify. There are near-universal reports of feelings of grief, anxiety, fear, and suffering amongst the family of stillborn children, extending from the affected parents to include extended family and any surviving or future children. Reports of chronic pain, fatigue, and increased substance use are also common, as are instances of relationship strain and breakdown following stillbirth 6. Of particular harm seems to be the stigma which in many countries is still experienced by parents of stillborn children, who may feel that they are blamed or that their their feelings minimised by their communities.6
There are also emotional costs borne by health professionals involved in stillbirths, which can include feelings of trauma, stress, guilt, anger, blame, or fear of litigation or disciplinary action 6.
Similarly to the economic cost, there is also obviously the loss of the WELLBYs that would potentially have been experienced by the stillborn individual. Again, how much these are weighted is largely an individual decision, or at least would require philosophical and economic thought beyond the scope of this shallow review, but again could significantly alter the estimated importance of stillbirths.
However, there are sometimes positive impacts of wellbeing related to stillbirths, with some parents saying that it strengthened their relationship or their sense of meaning through campaigning or religious activities and health professionals sometimes reporting a sense of honour or privilege, the development of stronger professional bonds, or increased confidence 6.
There’s no clear gender discrepancy noted in which babies are likely to be stillborn. Stillbirths can be dangerous to the mother in and of themselves and are also made more likely by poor maternal health; as a result, many interventions aimed at reducing stillbirths look to improve the health of childbearing women and many interventions which improve the health of childbearing women also reduce the risk of stillbirth.
By definition, the primary victims of stillbirth are so young as to have not yet been born; the other most directly impacted individuals are likely to be parents of childbearing age, particularly those who are at the extremes of childbearing age and are therefore at increased risk of stillbirth.
There is clear geographical variation in the rate of stillbirths. Somewhere between 84-98% of stillbirths occur in low- and middle-income countries,with around half of the total number occurring in 6 countries- India, Pakistan, Nigeria, the Democratic Republic of Congo, China, and Ethiopia.2 The highest rates of stillbirth per total birth are in Guinea-Bissau, Bangladesh, Pakistan, Afghanistan and Ethiopia.7 Individuals who live in rural areas, distant from healthcare facilities, are most at risk, as well as those of low socioeconomic status and low education; this trend is notable even in high-income countries, where discrepancies in stillbirth rates between such groups still remains.8
Stillbirths are sometimes thought of as inevitable tragedies, but it seems likely that only a small minority of stillbirths- in the order of 10%- are caused by non-preventable congenital abnormalities.5 This does not necessarily imply that the remaining 90% of stillbirths can be prevented, but does at least give a very high upper bound on the proportion which are potentially avoidable; a review of around 900 stillbirths in India and Pakistan suggested that around 75% were preventable9, which may be a more reasonable upper limit.
Without a gears-level understanding of the problem developing appropriate solutions is hard, but substantial work has been done on exploring and assessing the impactfulness of a limited range interventions aimed at reducing stillbirths, primarily those which take place during the antenatal period of the index pregnancy. Several authors10–12 arrived at similar “menus” of potential high-impact interventions, with small variations between authors, after assessing a wider pool for potential cost-effectiveness, with this set being taken from the 2016 Lancet series6:
| Group | Intervention |
| Preconception nutrition interventions | Balanced energy and protein supplementation
|
| Folic acid supplementation | |
| Micronutrient supplementation | |
| Basic antenatal interventions | Prevention and treatment of malaria |
| Detection and treatment of syphilis | |
| Tetanus toxoid immunisation | |
| Advanced antenatal interventions | Treatment of hypertension during pregnancy |
| Treatment of diabetes during pregnancy | |
| Treatment of foetal growth restriction | |
| Induction of labour at or beyond 41 weeks gestation | |
| Interventions during childbirth | Antenatal steroids for preterm labour |
| Antibiotics for preterm rupture of membranes | |
| Active management of third stage of labour | |
| Neonatal resuscitation |
This “menu” comprises the most well-investigated set of interventions and as such will be the focus of this review. However, it’s worth remembering that interventions to, for example, reduce poverty, increase access to education, or treat tropical diseases are likely to include a reduction in stillbirths as part of their wider impact, possibly a greater reduction than what can be achieved with interventions described here.
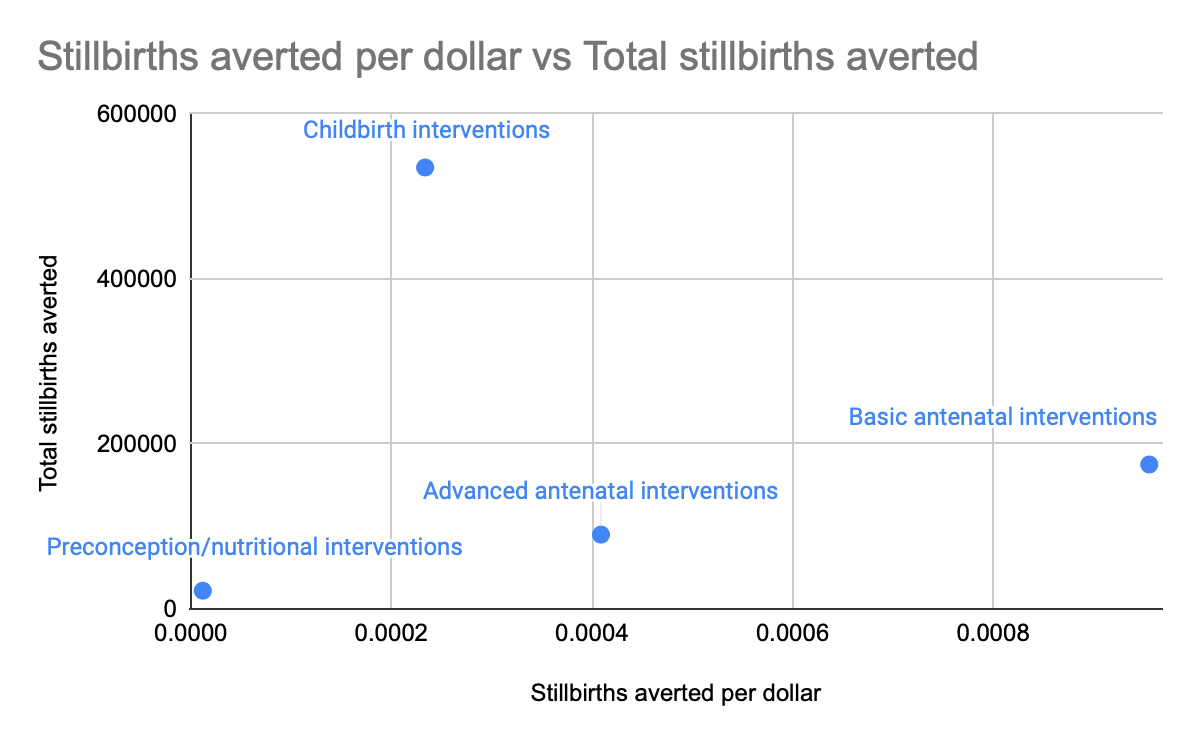
Despite the narrowness of their scope, this set of interventions has the potential for significant impact; scaling up their availability as a package in those countries worst affected by stillbirths to 90% is estimated to prevent 823,000 stillbirths, 1,145,000 neonatal deaths, and 166,000 maternal deaths each year for an additional cost of $4.6billion. If stillbirths prevented are considered to be lives saved, this gives an estimated cost of $2143 per life saved, competitive with the lowest values achieved by Givewell Top Charities.6
The majority of the stillbirth reductions from the implementation of these interventions comes from those aimed at childbirth, although this group is by an order of magnitude the most expensive if implemented as described.
The most cost-effective interventions are those in the basic antenatal group. These are estimated to avert a stillbirth, maternal, or neonatal death at a cost of $830 per life saved6, although the number of lives which can be saved at this price is likely to be limited. These interventions also have an outsized reduction in stillbirths relative to the number of lives they save, if we are looking for interventions which specifically reduce stillbirths; in particular, it looks like the treatment of syphilis and the induction of labour that continues past 41 weeks might be interventions with unusually high impact on stillbirths in particular.13
These general trends seem to be well replicated throughout the literature; for example, an earlier review in 201110 and a Cochrane review in 202012 arrived on a similar set of promising interventions at similar levels of cost-effectiveness. However, it seems worth focusing particularly on those two interventions as being particularly promising in our goal to reduce stillbirths.
In some ways, these two examples illustrate to me the two “classes” of intervention in stillbirths that effective altruists might consider pursuing. Antenatal syphilis can be treated effectively with a single course of a generic antibiotic called Penicillin G, leading to a reduction of stillbirth risk of approximately 82%14. Although there have been concerns about the availability of Penicillin G in some developing countries, the cost-effectiveness of this intervention- estimated to be around 10$ per DALY saved- has led to investment from mainstream EA organisations in the past, as outlined below.
Scaling up the availability of induction at labour represents a very different challenge to procuring, distributing, and administering single doses of antibiotics. Although the induction of labour in itself is not technically difficult, usually involving the administration of misoprostol, the decision to induce is one usually taken by highly trained healthcare professionals like obstetricians and midwives within a fairly advanced healthcare facility. Therefore, the availability of induction depends not simply on the availability of a single drug but on the creation and maintenance of a sophisticated healthcare facility with trained staff, with all the upfront costs which that requires before any health benefits begin to be accrued.
The induction of labour, therefore, might be more reasonably considered as a part of the toolkit of a wider but still promising intervention- the availability of midwives to attend births. Work to assess the impact of midwife availability on stillbirths is promising, although suggests that most of the reduction comes only once nearly full coverage is achieved, whereas significant reduction of maternal and neonatal death seems to come with more modest coverage.15 It’s not clear why this would be, and without more data on what midwives do and which of their actions are most impactful it’s hard to evaluate the cost-effectiveness of midwives as an intervention in and of themselves.
The available literature can also guide us as to what interventions are unlikely to be significantly cost-effective, some of which can be surprising. For example, magnesium is often used to treat pre-eclampsia (a potentially fatal maternal illness) in the developed world, but magnesium was found not to significantly reduce the rate of stillbirth or perinatal death in randomised trials.10 Smoking is a commonly cited risk factor for stillbirths, but there is no strong evidence to suggest that interventions to aide smoking cessation during pregnancy reduce the risk of stillbirth.12
Many of the world’s largest health organisations, including national governments and international bodies, have declared their intentions to reduce stillbirths. In many cases, this takes the form of a national commitment to the Every Newborn Action Plan, which was developed by the World Health Organization16 and endorsed by 194 nations in 2014. However, around 25% of the nations endorsing the Plan are not on track to achieve its goals2, and it may be that this gap could increase the appeal of EA-led interventions to local governments who have already made political commitments to reducing stillbirths.
There are also large non-governmental organisations who contribute financially to global stillbirth reduction. The Bill and Melinda Gates Foundation, at the time of writing, have given 8 grants directly towards stillbirth reduction, with the largest being the $20,000,000 donation to the Global Alliance to Prevent Prematurity and Stillbirth. It seems likely that many of their other grants have gone towards work which reduces stillbirth-for example, a $40,000,000 grant to the WHO to “strengthen rapid scale up of Maternal, Neonatal, and Child Health interventions in Africa”, which intentionally or not are likely to reduce stillbirth risk.
In high-income countries, many large charitable organisations spend significant amounts of money on stillbirth; SANDS, the leading stillbirth charity in the United Kingdom, spends several million pounds a year, with similarly sized charities operating in the United States. Detail on where or how these organisations spend their money, however, is difficult to obtain.
Funding has also been directed toward stillbirth reduction from within the EA community. GiveWell has directed just under $20,00,000 to Evidence Action to fund their work on syphilis testing and treatment in pregnancy- see below for details.
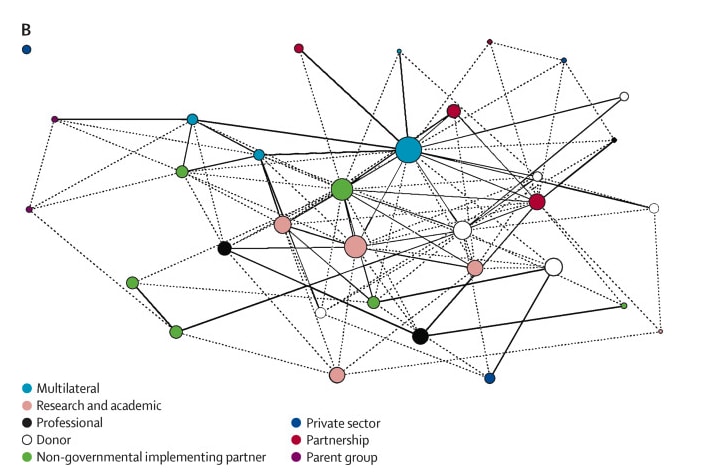
Mapping exercises of organisations involved in global stillbirth prevention demonstrate the tangled web of academic, charitable, governmental, and private sector bodies involved5:
It is therefore difficult to highlight which organisations in particular are dominant in actually implementing interventions to reduce stillbirths; in many countries, national governments are responsible for the direct work of stillbirth reduction via their health systems, often with an ecosystem of charitable and academic bodies fulfilling research functions and providing support to those affected by stillbirth.
It may be more feasible to search for those bodies implementing the two particularly promising interventions mentioned earlier, antenatal syphilis treatment and induction for post-term labour. Evidence Action is working in Liberia, Zambia and Cameroon to help them reduce antenatal syphilis by adding syphilis tests to the existing HIV screening programme.
My broad conclusion from this shallow review is that stillbirth reduction is likely to be very important, moderately tractable, and not particularly neglected. Although there are promising potential interventions, many of the highest-yield routes to stillbirth reduction are probably best executed by local and national health services, rather than smaller organisations, as they have their most significant impact at large scale.
Many organisations, like those involved in treating HIV or malaria, already target interventions which are likely to reduce stillbirths as a positive but potentially undervalued side-effect. It may be the case that formalising a method for including the harms of stillbirths would significantly alter our thinking on which global health interventions are likely to be most cost-effective. Work on describing and incorporating the harms of stillbirth seems important and promising.
Outside of the traditional ITN framework, there may be additional benefits arising from a reduction in stillbirths. Economic growth is a function at least partially of population growth, and thus may well be improved by fewer stillbirths; in an ideal world, this could contribute to a “virtuous circle” of economic growth and improving health.
Stillbirth reduction is also a legible cause area to those outside of the EA movement and success might therefore be positive for our reputation beyond its “pure” impact. Given the cohort of people most affected, stillbirth reduction is likely to appeal to individuals interested in social justice and equity, who are sometimes suspicious of the EA movement, and coordination with these and other groups might make EA more effective in the future.
Less prosaically, it can be easy to become inured to the true stories which lie behind quantitative estimates and dry economic analysis of human lives and deaths. I’m deeply lucky to be able to do work which acknowledges the sanctity and preciousness of human life, and I’m glad to be part of a community which is so committed to celebrating and carrying out that intuition in everyday life.
Huge thanks to Cause Innovation Bootcamp, Leonie Falk, Akhil Bansal, and Vicky Cox for coordinating and giving feedback- any errors are mine.
1. World Health Organization. Stillbirth [Internet]. Available from: https://www.who.int/health-topics/stillbirth
2. UN Inter-agency Group for Child Mortality Estimation. A Neglected Tragedy- The global burden of stillbirths [Internet]. 2020. Available from: https://platform.who.int/docs/default-source/mca-documents/maternal-nb/a-neglected-tragedy-stillbirths-igme-report-english-2020.pdf?Status=Master&sfvrsn=13cfa3f6_4
7. UN Inter-agency Group for Child Mortality Estimation. CME Info - Child Mortality Estimates [Internet]. Available from: https://childmortality.org/
11. Are stillbirths stillborn on the global agenda? [Internet]. Available from: https://www.countdown2030.org/documents/Stillbirth_Globalagenda_Blencowe.pdf
12. Erika Ota, Katharina da Silva Lopes, Phillipa Middleton, Vicki Flenady, Windy MV Wariki, Obaidur RAhman, et al. Antenatal interventions for preventing stillbirth, fetal loss and perinatal death: an overview of Cochrane systemic reviews. Cochrane Database Syst Rev [Internet]. 2020 Dec 18;(12). Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD009599.pub2/full
16. Every Newborn Action Plan [Internet]. [cited 2022 Dec 9]. Available from: https://www.who.int/initiatives/every-newborn-action-plan


In addition to the $3.9M grant, there's also a more recent $15M grant to scale up.
I was surprised to read that GiveWell estimates the value of "averting stillbirth or miscarriage" at 21 (where 1 is the value of doubling someone's income for 1 year) and the value of averting a stillbirth at 33 based on a survey of "70 of our largest donors", sadly it seems that they didn't have beneficiaries survey data on the value of preventing stillbirths.
That's more than what I would have guessed (for reference, the value of "preventing one 5-and-over death from malaria" is 83).
Thankyou for this- I've updated the post. I think this particular narrow intervention (adding syphilis testing to routine HIV screening programmes) is super exciting.
Interesting. What would your guess have been? My instinct is that people will have a very wide range of intuitions on this, at least until we're able to be a bit more specific about what we're asking for- even then, I expect quite a high degree of variance in how much people value averting a stillbirth. I don't have a strong opinion myself on what the right number is.
I agree with this, and I think this might be a case where the largest donors, median donors, and beneficiaries might have very different intuitions.
Very low confidence, but my central estimate would have been closer to 10, when asking beneficiaries, but it's a baseless wild guess based on nothing.
Agreed that this seems very possible. Who should we listen to most closely if it is the case?