Thanks for writing this up, and congrats on having preliminary promising signs!
I left a bunch of more minor comments in the CEA sheet (thanks for making that public).
Are there any interest groups on the other side of this issue? I suppose budget hawks and fiscal conservatives may try to shoot down any new funding plan, particularly given EU budgetary woes. But otherwise, it seems like a good issue in terms of not making powerful enemies (since the Pharma industry is onside).
This post is co-authored with Ben Garfinkel. It is cross-posted from the CEA blog. A PDF version can be found here.
Summary: Some strategic decisions available to the effective altruism m...
Disclaimer: Although I work on the Groups Team at CEA, I’m writing this in a personal capacity, and this post does not constitute an endorsement by CEA.
Agency - the realisation that you really can just do things.
TL;DR
Biosecurity needs people (of any background) who are agentic and have a high execution velocity and track record....
Summary
Making AI safe and good requires many people to be ready to address crucial problems. However, our current “pipelines” for finding, training, and accelerating talented individuals who could work on these problems are “leaky”, meaning there are many ways they can be improved. This post shows my full overview of the AI safety talent pipeline: where people come from, where they go to learn more, and why this is impactful. I also describe some “leaks” in the pipeline: stages that...
It’s been just over a year since ARMoR launched through the CE/AIM incubation program! In that time, we’ve worked hard to push for policies that will help tackle the rising threat of antimicrobial resistance (AMR) and made some strong progress towards this aim.
As part of our anniversary, we want to take the opportunity to:
Explain why AMR is so important
Share a little about how our first year has gone
Make the case for why our work is worth supporting
Please contact us at [email protected] if you have any questions, comments, feedback, or are interested in donating!
TL;DR
Antimicrobial resistance is a serious global health threat.
We need a continuous pipeline of new antimicrobials coming to market to replace those which are no longer effective.
Market incentives have failed to stimulate the needed innovation.
ARMoR works to implement these policies through a combination of research, advocacy, and informational lobbying.
Our first year of operations has updated us favourably on the neglectedness and tractability of this intervention.
We conservatively estimate that our work has a cost-effectiveness of about $950 per life saved globally and $6,200 per life saved when just considering the EU.
We are looking to raise an additional $420K to support our next two years of operations, with a minimum need of $149K to support us for the next year.
Marginal funding towards these targets would be very useful.
Thank you for your time and consideration!
Antimicrobial resistance is a looming global health crisis
The growing health burden of antimicrobial resistance
Since the discovery of penicillin in the early 1900s, antimicrobials have played a pivotal role in ushering in the age of modern medicine. These drugs not only significantly reduce the burden of infectious diseases on our healthcare systems but also enable us to perform life-saving surgeries, administer chemotherapy, and manage chronic illnesses. Because of antimicrobials, many of us no longer have to fear dangerous infectious diseases like tuberculosis, sepsis, and meningitis.
Unfortunately, the antibiotics that have protected humanity for decades are losing their effectiveness. Already, one million deaths are directly attributable to AMR globally every year. This ranks it among other major global health threats such as malaria (at ~650,000 deaths/year) and Tuberculosis (at ~1.2 million deaths/year). The kicker is that unlike Malaria and Tuberculosis, whose disease burden is shrinking every year, the disease burden of AMR is steadily growing. Without serious intervention, it is projected that by 2050 the number of deaths due to AMR will double to 2 million deaths annually.
We can combat this rising threat on two main fronts:
Reduction of the rate at which bacteria (and other microbes) develop resistance.[1]
Development of new antimicrobials that are effective against resistant infections.
Given how poorly understood the drivers of resistance are (see this paper for more), and the fact that it seems unlikely that we'll be able to reduce the growth of resistance in the short term though stewardship efforts, focusing on the development of new antimicrobials seems to be a more robust and tractable option to reducing the burden of AMR.
The market failure preventing antibiotic development
One reason that the malaria vaccine took so long to develop, despite its immense social value, is the fact that most of the beneficiaries have a limited ability to pay. Like malaria, low and middle income countries bear the majority of the AMR health burden, accounting for nearly 90% of the direct death toll. Unlike malaria, AMR is an issue everywhere, claiming more than 35,000 lives every year in the EU/EEA.
With a large (and growing!) death toll in the west, you might expect there to be a strong financial incentive for companies to develop new life-saving antimicrobials that circumvent resistance. Unfortunately, this has proven not to be the case.
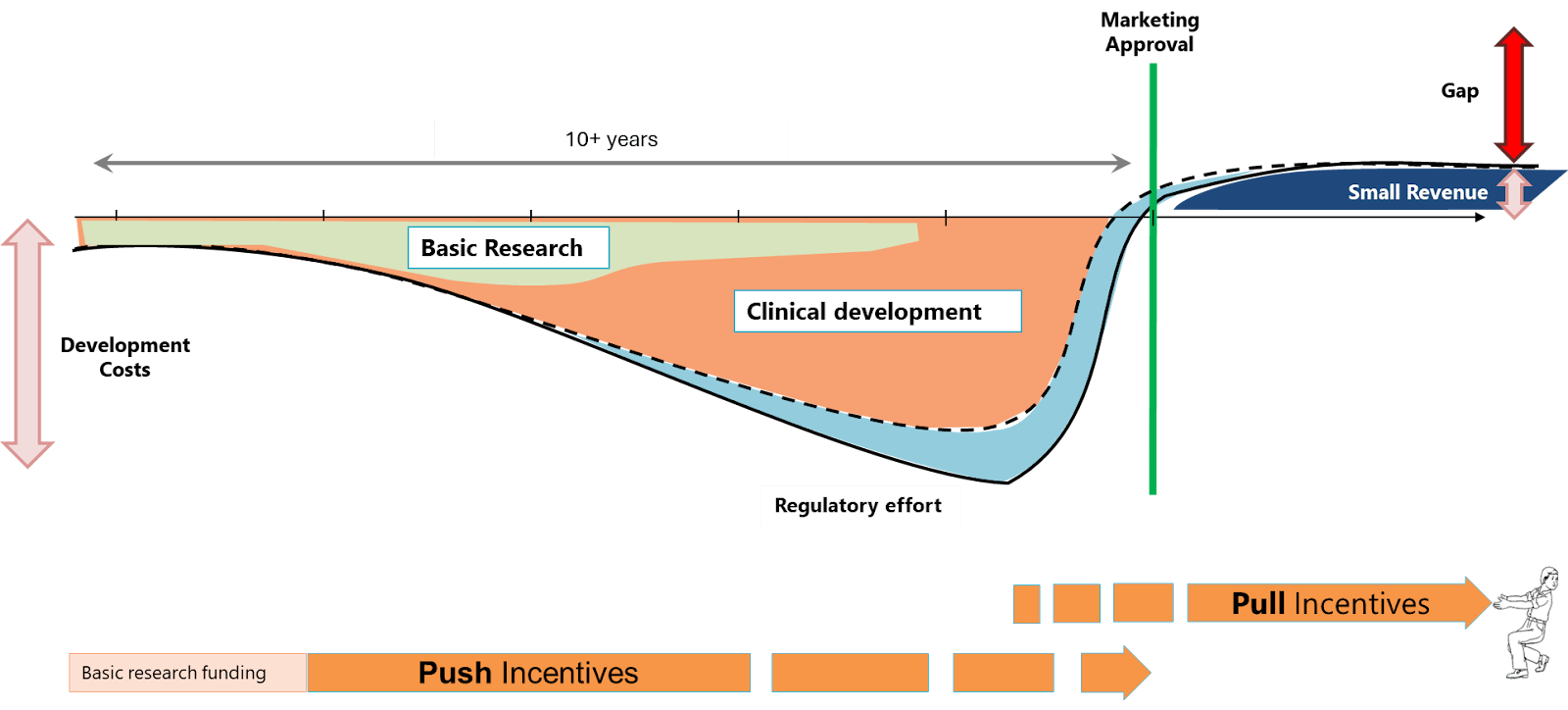
New antibiotics are incredibly expensive to research and develop. The cost of getting a novel antibiotic to market is estimated to be upward of one billion dollars. However, once developed, payers are incentivised to drive down the cost of the antibiotics while health care professionals aim to use new antibiotics as sparingly as possible to prevent the growth of resistance. These issues are further compounded by the fact that clinical trials and traditional governmental reimbursement mechanisms aren’t well-suited to evaluate antimicrobials. [2]
The development of novel antimicrobials is a classic case of a market externality: the societal value of antimicrobials far exceeds the revenue they bring in.
The cost of development of a new antimicrobial far outweighs the expected revenue
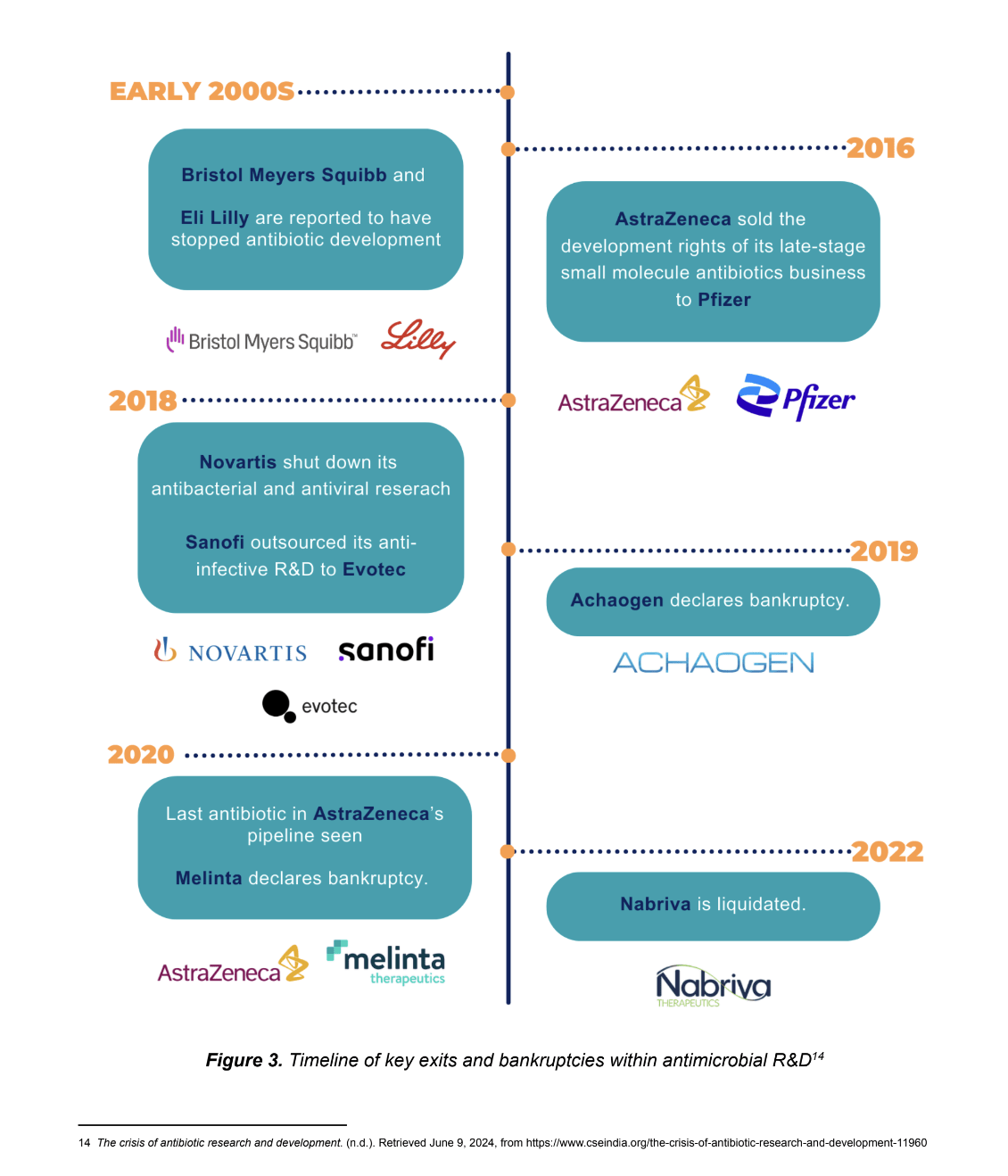
Most large pharmaceutical companies have now shut down or sold off their antimicrobial R&D divisions, and much of the skills and expertise that were built up there is lost. Since 2019, three important companies which specialised in antimicrobial development have declared bankruptcy. The pipeline is now mostly in the hands of small and medium biotech companies, who often lack the needed investment and resources.
Without urgent change, we are looking at the complete collapse of the antimicrobial pipeline within the next 10 years
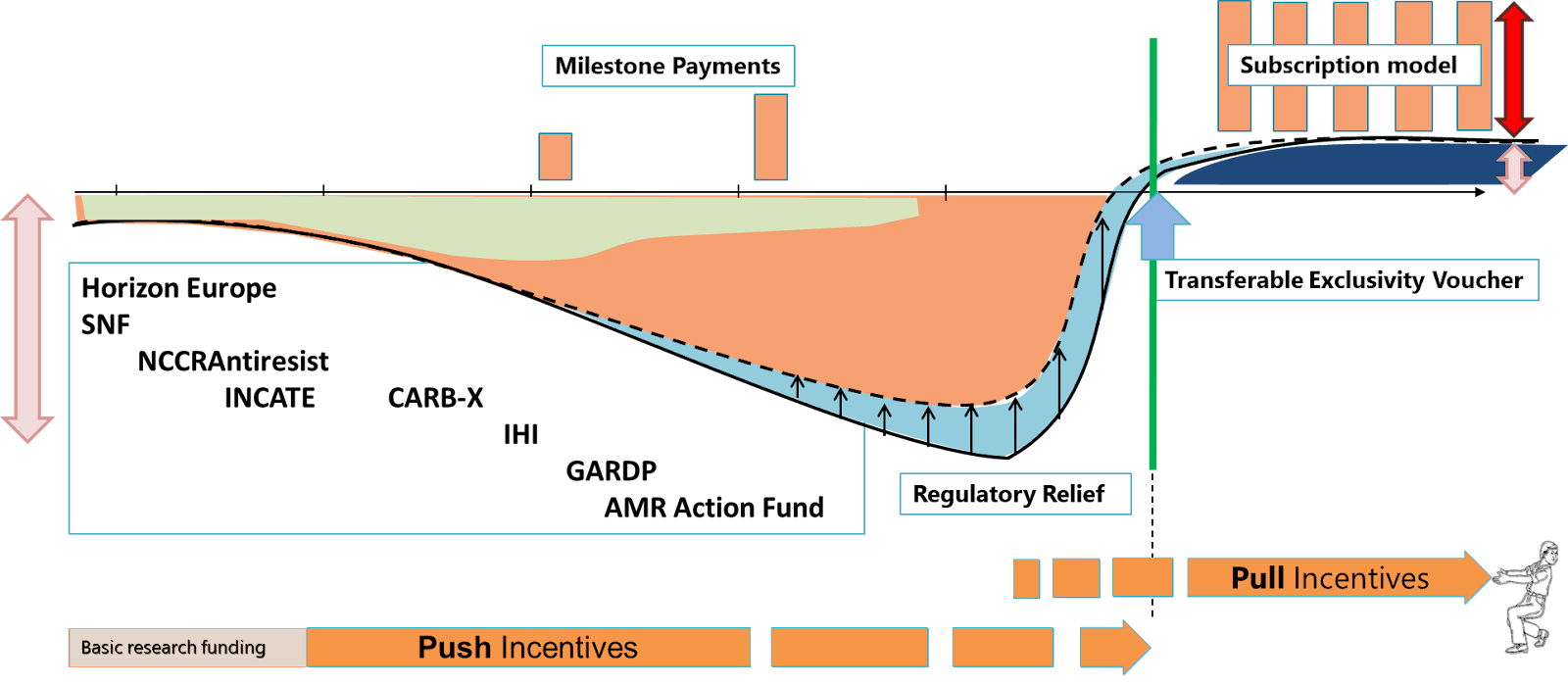
Fixing the market failure with pull incentives
For new antibiotics to be developed, it has to become profitable to do so.
We advocate for policies which make this possible. In particular, we believe that pull incentives are an effective mechanism to achieve this.
Pull incentives (such as advance market commitments) offer innovators a guaranteed revenue for bringing novel antimicrobials to market. For antimicrobials this revenue should ideally be independent of sales volumes, so pricing can be based on appropriate use rather than profit. If governments pre-commit to paying a sufficiently high enough price before the drug is developed, companies can safely pay the R&D cost knowing that they can receive a reasonable return on investment (ROI) once the product is approved. [3]
Pull incentives align the expected revenue of bring new antimicrobials to market to represent the societal value of these drugs
The issue, however, is that pull incentives are quite susceptible to global coordination and “free rider” problems. Governments have recognized the need for innovation in this space, but for any single country, the value of a new antibiotic is lower than the total R&D cost. This means that in order for pull incentive policies to be a good investment, enough countries must be brought into the idea. This issue is further compounded by the need for upfront funding and the fact that any single country which puts out an advance market commitment to incentivize development, would effectively be subsidising the drug for all other countries who will try to bargain the price down to its marginal cost of production.
These challenges make implementing pull incentives difficult, but not impossible. In fact, several countries—including the United Kingdom, Sweden, Japan, and most recently Italy—have introduced versions of this policy. The United States, the EU, and other nations are also in the early stages of exploring similar approaches. However, progress remains slow, and if we want to avoid a pipeline collapse, a more concentrated effort is essential.
Global Access and Stewardship Conditionalities
Given that the majority of the AMR burden falls on low- and middle-income countries (LMICs), it is essential that any implemented pull incentive policies include mechanisms which can support access and stewardship in these regions. These conditions can be built into pull incentive models and would ensure that incentives are awarded only if innovators commit to specific guidelines on access and stewardship. For instance, developers might be required to provide new antimicrobials to LMICs at affordable prices or agree to licence the drug to third parties serving LMIC markets.
Our first year: research, advocacy, and informational lobbying
Our work is predicated on two main assumptions:
Small increases in the chances that pull incentive policies are implemented is highly cost-effective (ie. has a high expected-value of impact)
A small-scale, start-up NGO with limited expertise and resources (ie. ARMoR) is able to exploit opportunities that lead to small increases in the chances that an EU-wide pull incentive is implemented
If either of these assumptions are proved likely to be false, it would mean that ARMoR should seriously consider shutting down or pivoting to a more impactful area.
Before launching ARMoR, we were relatively confident in the first assumption. However, we had far less confidence in the second. Specifically, we were uncertain about the following:
Neglectedness: Antimicrobial resistance is a well-known global health threat with seemingly many actors working in the space. Would there be space for an additional actor? Would the marginal impact of this additional actor be impactful? Would this policy get passed with or without us?
Tractability: Would a small organisation working on pull incentives be listened to? Would we be able to “get in the room”? Would we be able to build the credibility to influence meaningful change?
In many ways, we viewed our first year of operation as a time to test these key uncertainties and make sure that ARMoR was indeed a good long-term investment. We’re now much more confident in our ability to have an impact in this space.
First, although governments have taken initial actions towards the implementation of pull incentives, there is still a lot of work to be done. For example, in the recent deliberations over the EU pharmaceutical legislation, a type of pull incentive called a ‘transferable exclusivity extension” is being negotiated. This policy would allow developers of new antibiotics to extend the “patent” of another more profitable drug in their lineup, as a way to encourage and increase the profitability of bringing new antibiotics to market. However, not only is this mechanism quite far from being passed, we believe that there are serious issues with the design of the policy which would significantly reduce its effectiveness.
While there are several actors working on this issue, many of the main actors in this space are industry organisations who aren’t as trusted by policymakers and benefit directly from the policies being passed. Meanwhile, global health organisations typically have a much broader focus and don’t have the detailed expertise needed to advocate for these specific policies. In some ways, we think that the need for additional actors is demonstrated by the lack of research, advocacy, and lobbying efforts on global access conditionalities.
Given this, we believe that there is a lot of value in positioning ourselves as non-industry affiliated “experts” on pull incentive implementation. In particular, we believe that advancing this agenda requires more stakeholders (like ARMoR) to:
Keep building momentum by putting constant pressure on policymakers to keep working on this issue
Create and disseminate resources policymakers need to take the next steps towards a solution (detailed implementation guidelines and research, etc.) and reduce the friction for governments to do so
Act as coordinators and accountability mechanisms, helping countries align on the best course of action and feel more confident that their country won’t be taken advantage of (free rider problem).
In terms of tractability, despite being a new and small organisation, ARMoR has established credibility and engaged with a wide range of stakeholders. Over the past year, we influenced the EU Parliament’s stance on antimicrobial pull incentives, successfully incorporating language on subscription models and global access into draft legislation. We have also taken a leadership role, coordinating a coalition of influential NGOs to create a unified policy position on EU pull incentives, and one of our co-founders was invited to present on these incentives to Member State stakeholders at a European Commission training session. Additionally, our recent cost-benefit analysis on EU pull incentives has been used in discussions with over ten governments, further bolstering our network of contacts across the European Commission, Parliament, and Council representatives.
Overall, because the declining antimicrobial R&D pipeline is an issue with a broad level of consensus among policymakers, we think this issue, despite being a large policy task (moving potentially billions of dollars and requiring large amounts of global coordination) is more feasible than other interventions on a similar scale.
Programs, Progress, and Next Steps
Right now, most of our work can be divided into four main workstreams: European Union campaign, Nordics campaign, member state outreach, and global access research. The rest of this section will outline the objectives and rationale for each of these programs as well as some highlights of the progress we have made and our planned next steps.
It’s a little in the weeds, so feel free to gloss over. We also have a recent newsletter which goes over some of this at a higher-level.
European Union campaign
Objective(s): work with the Council of the EU, Commission, and Parliament (and other relevant stakeholders) to push for suitable pull incentive, to be included in the ongoing updates to the EU pharmaceutical legislation or alternative policy vehicle.
Rationale: pull incentives only work if there is enough global buy-in. Given the size of the EU, their implementation of these policies would contribute a significant portion of the total incentive amount needed. Furthermore, the conversation around pull incentives in the EU is quite "hot" given the discussions surrounding the EU general pharmaceutical legislation.
Highlights:
Engagements with all major parties in the European Parliament, leading to the inclusion of a requirement for global access planning in their position on the general pharmaceutical legislation
Giving a presentation on pull incentives to Member State representatives as part of a Commission training session
Building a strong stakeholder network of NGOs within the Brussels global health space
Next Steps:
Continue to engage with EU institutions to push for the adoption of pull incentives, including developing more technical details to support our proposal
Publish a joint position paper with our NGO collaborators
Support in coordinating discussions between Member States, possibly through hosting an event in 2025
have Nordic representatives support and champion initiatives to implement flexible revenue guarantee models at an EU-wide level
have Nordic countries include commitments to investigate innovative financing mechanisms to stimulate antimicrobial R&D in their National Action Plans on AMR
Rationale:
The Nordics countries have demonstrated a relatively high level of interest in these types of policies and have precedence for working together for the joint-procurement of drugs through the Nordic Pharmaceutical Forum. Given the need for collaboration on pull incentives to ensure sufficient funds, a collaborative effort to implement a pull incentive in these countries might be promising.
These pilots can serve as a valuable proof-of-concept, demonstrating the effectiveness of pull incentives and showing policymakers at the EU that member states will buy-in to a coordinated EU-wide scheme.
In order for an EU-wide pull incentive scheme to be implemented, member states will need to figure out how the system will be funded/implemented at the national level. If some member states have already run pilots and figured the process out, this transition will occur at a much faster rate.
Highlights:
We were invited by the UK Science and Innovation Network to give a keynote presentation at an event on “Galvanising AMR finance”, an event hosted by the UK for Nordic and Baltic countries, specifically looking at pull incentives.
Published policy briefs on the ROI of pull incentives in Norway, Denmark, and Sweden in collaboration with in-country partners.
We collaborated with the Danish AMR Alliance, a group of industry and academic experts including Pfizer and Novo Nordisk, who incorporated our ROI figures and recommendations into a policy proposal which they submitted to the Danish government.
Next Steps:
Establish an active Nordics MP Group on AMR based on the German MP group on AMR. The purpose of this group would be to bring together MPs interested in this issue and give them the resources needed to advocate on behalf of effective AMR-related policies.
Build a coalition of relevant stakeholders (industry, patient groups, NGOs, health care professionals, etc) to advocate for policies, specifically pull incentives mechanisms, that will help build a more sustainable ecosystem for high-value antimicrobials in the Nordics.
Build connections with policymakers and investigate how a pull incentive could be coordinated at the Nordic level, ideally building off of existing legal/logistical processes
Member state outreach
Objective(s): Build strong relationships with policymakers in charge of AMR in various EU institutions member states. Aiming to act as an advisor to them and provide them with the research, information, and connections needed to make decisions.
Rationale: Despite ongoing discussions on the for new R&D and access incentives for antimicrobials at the EU level, policymakers within individual EU member states often lack a reasonable understanding of the issue. This knowledge gap poses a significant challenge, as these policymakers are crucial to the successful passage and implementation of a built into the design of pull incentive mechanisms in EU countries
Highlights:
ARMoR recently published a cost-benefit analysis on pull incentives in the EU which has been used by ourselves and collaborators in discussions with 10+ governments including at the G7 ministerial level. The Office of Health Economics (a leading think tank) endorsed and wrote a blog about this work.
We partnered with the Global Antibiotic Research and Development Partnership (GARDP) to write an official policy brief for the 2024 G7 Summit. As a supplement to this report, we performed compliance evaluations together with the University of Toronto, G7 Research Group utilising their academic framework to assess each G7 country's adherence to commitments on AMR.
We were recently asked to submit evidence to the German Bundestag subcommittee on health for a session that they are having on AMR.
Published an article in the Business Post on the benefits of market-shaping mechanisms and AMR.
Next Steps:
Work in member states on an opportunity driven basis, for example, to influence election manifestos/updated national action plans on AMR.
Conduct a landscape analysis which brings together data and resources relating to AMR in individual member states. This will ideally serve as a resource for other advocates to push for pull incentives in their countries.
Global access research
Objective(s): Build a better understanding of what LMIC access conditionalities should look like and push for their implementation. Generally explore ideas for potentially cost-effective interventions to improve global access to antimicrobials.
Rationale: Given that the majority of the AMR burden falls on low- and middle-income countries (LMICs), it is essential that any implemented pull incentive policies include robust global access and stewardship conditions.
Highlights:
SECURE is a WHO/GARDP initiative aimed at improving access to new and existing antimicrobials. We are currently working with them to investigate the cost-effectiveness of improving access to various antimicrobials and hope to be able to share more information about this work in the near future. SECURE has funded us to continue with this work (regrant from Gates Foundation).
We drafted an open letter to EU institutions and member states, outlining reasonable and expected conditions for recipients of pull incentives. Although still in its initial stages, we have secured key signatories and we hope that this letter will help set standards in the EU and serve as a template for other countries implementing their own pull incentive schemes.
Next Steps:
Publish a paper on the different types of global access conditionalities and how to implement them.
Investigate different potential interventions and policies relating to antibiotic access.
Cost-effectiveness of AMR advocacy
Due to the nature of policy work, cost-effective analyses are inherently somewhat speculative and based around low chances of very high amounts of impact. ARMoR is no exception, but we’ve done our best to model the expected impact of our work, aiming to be quite conservative to balance out the higher levels of uncertainty.
Our current analysis, based on Founder Pledge’s methodology for evaluating policy organisation, shows that work pushing (a blanket term encapsulating a combination of research, advocacy, and informational lobbying) for pull incentives in the EU has a cost-effectiveness of about $950 per life saved globally and $6,200 per life saved when just considering the EU.
We calculated these numbers under the assumption that ARMoR, alongside other actors in the space, have a 10% chance of speeding up the passage and implementation of an EU-wide pull incentive by one year and improving the design of the mechanism such that an additional 6.5 new antimicrobials are created in expectation. Furthermore, given our current understanding of the AMR R&D ecosystem, we give ourselves a 7.5% attribution of the total impact this “policy win” would have.
Beyond these numbers, a big part of our work right now is helping policymakers understand pull incentive schemes and the value they bring. Although our work is mostly in the context of new antimicrobials, we believe that increasing policymakers' familiarity with the general idea of pull incentives is a big win. As shown by the work being done by the Chicago Market Shaping Accelerator, there are several different opportunities for pull incentive policies to have a significant impact, particularly in the areas of pandemic preparedness and climate resilience. These policies might have a smoother pathway to implementation if many relevant policy makers are already familiar with the core ideas and have a clear example of a pull incentive being implemented.
The impact of Marginal Funds
As our current campaigns scale-up, we are looking to raise an additional $420K to support our next two years of operations, with a minimum need of $149K to support us through 2025.
Here are some examples of what different amounts of marginal funding contributions towards this target would allow us to accomplish:
$10,000 → funds an extra month of full-fledged operations
$34,000 → funds a full-time research hire for one year
So far, our research outputs have been responsible for some of our most promising leads and opportunities
$48,000 → funds an in-country, on-the-ground contractors with strong policy advocacy/lobbying experience
In general, we believe ARMoR is susceptible to the “bystander effect”. In other words, our work falls at the intersection of global health and biosecurity, leaving us in a grey-area where it’s not clear who our main funders will be. Marginal funding will give us more time to establish ourselves, thereby increasing our chances of securing more substantial core funding in the future.
Conclusion
Overall, while there are still significant uncertainties, our first year has updated us favourably on the neglectedness and tractability of this intervention. We believe that ARMoR is a good bet if you want to cost-effectively save lives and reduce the growing burden of antimicrobial resistance.
Please reach to [email protected] if you have any questions, comments, feedback, or are interested in supporting our work! Thank you for your time and consideration!
This can be done through better infection prevention and control, WASH interventions, improved agricultural practices, improved antimicrobial stewardship etc.
We specifically advocate for revenue guarantees, a pull incentive model offering developers a fixed annual reward based on the drug’s value to patients and the healthcare system. Under this approach, hospitals purchase the drug as usual, with prices structured to promote appropriate use. Each year, a “top-up” payment is made to cover the gap between sales revenue and the predetermined reward, ensuring developers receive consistent, value-based compensation.




Thanks for writing this up, and congrats on having preliminary promising signs!
I left a bunch of more minor comments in the CEA sheet (thanks for making that public).
Are there any interest groups on the other side of this issue? I suppose budget hawks and fiscal conservatives may try to shoot down any new funding plan, particularly given EU budgetary woes. But otherwise, it seems like a good issue in terms of not making powerful enemies (since the Pharma industry is onside).